

Gestational - age - specific reference intervals for blood pressure in normal pregnancy in a Southern Chinese population
- PMID: 39773091
- PMCID: PMC11706196
- DOI: 10.1186/s12884-024-07117-3
Gestational - age - specific reference intervals for blood pressure in normal pregnancy in a Southern Chinese population
Abstract
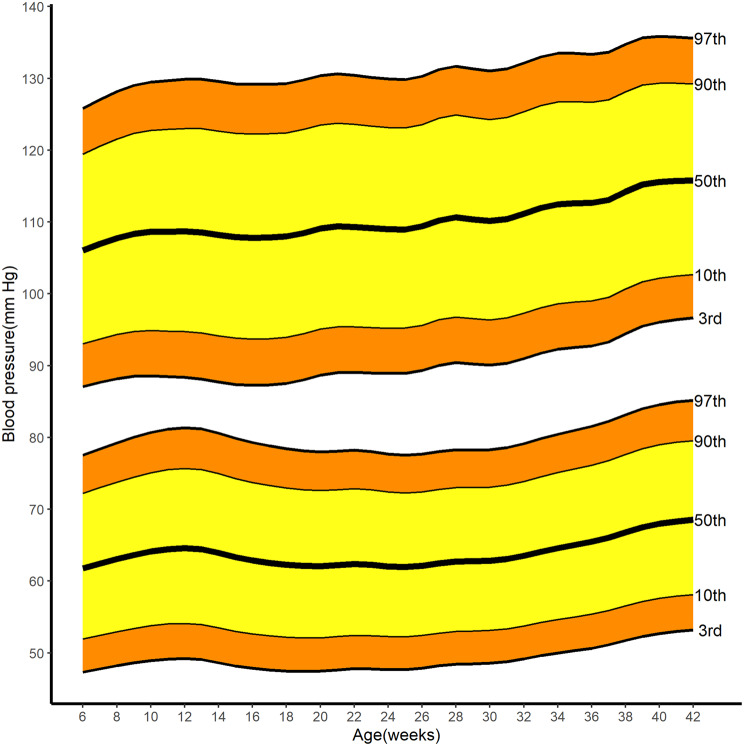
Objective: Physiological blood pressure changes in pregnancy are insufficiently defined. This paper describes the blood pressure changes across healthy pregnancies in a Southern Chinese population to present gestational - age - specific blood pressure ranges with smoothed centiles (3rd, 10th, 50th, 90th, and 97th).
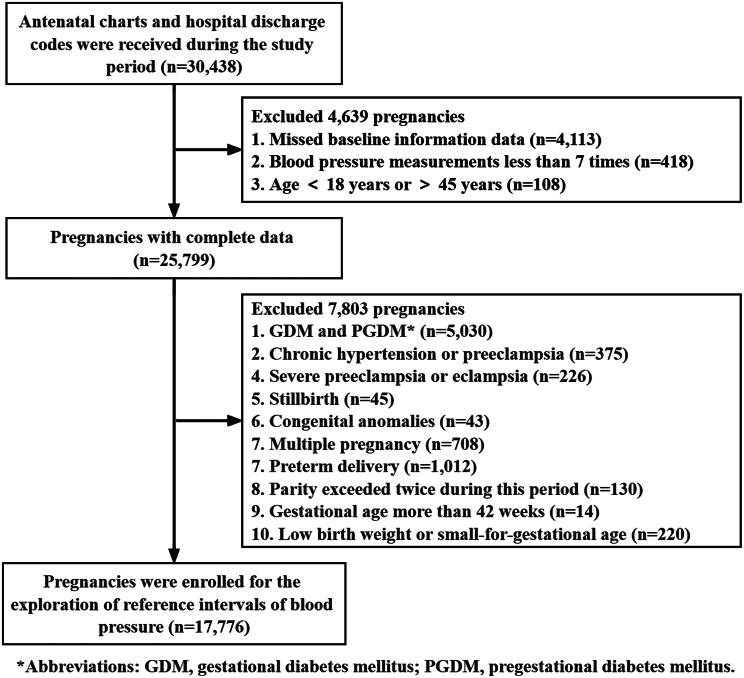
Methods: Antenatal blood pressure measurements [median (interquartile range) 9 (8 - 10) per woman] were repeated in 17, 776 women from a Southern China population. Multilevel cubic splines models were used to derive longitudinal reference ranges for systolic blood pressure (SBP) and diastolic blood pressure (DBP) from 6 to 42 weeks of gestation for the normal pregnancies (excluding chronic hypertension, preeclampsia, diabetic ones, and preterm birth et al.).
Results: Systolic and diastolic BP increased from 6 weeks of gestation: 50th centile (3rd - 97th centile) 106 (87 - 125); 61 (47 - 77) mm Hg to 12 weeks of gestation: 50th centile (3rd - 97th centile) 108 (88 - 129); 64 (49 - 81) mm Hg. Then, the lowest value of 107 (87 - 129); 62 (47 - 78) mm Hg was reached at 16 weeks and 20 weeks of gestation, respectively. Systolic and diastolic BP then rose to a maximum median (3rd - 97th centile) of 115 (96 - 135); 68 (53 - 85) mm Hg at 42 weeks of gestation. Additionally, the ascending tendency of SBP after 16 weeks of gestation was interrupted by two fluctuations that occurred at 24 weeks and 30 weeks of gestation.
Conclusions: In summary, our study provides blood pressure reference values for Southern Chinese women with normal pregnancies. To identify gestational hypertension and hypotension, centiles for gestational - age - specific BP should be defined in healthy pregnancies. Understanding these changes in low risk pregnancies is essential to optimize maternal blood pressure management.
Keywords: Blood pressure trajectory; Normal pregnancy; Reference intervals.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study has ethical approval from the Longgang District Maternal & Child Healthcare Hospital Research Ethics Committee (No. LGFYYXLLL-2022-016). All participants have signed the written informed consent. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Say L, Chou D, Gemmill A, Tuncalp O, Moller AB, Daniels J, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323–33. - PubMed
-
- Reddy M, Rolnik DL, Harris K, Li W, Mol BW, Da Silva Costa F, et al. Challenging the definition of hypertension in pregnancy: a retrospective cohort study. Am J Obstet Gynecol. 2020;222(6):e6061–21. - PubMed
-
- Warland J, McCutcheon H, Baghurst P. Maternal blood pressure in pregnancy and stillbirth: a case-control study of third-trimester stillbirth. Am J Perinatol. 2008;25(5):311–17. - PubMed
-
- de Los Reyes S, Plunkett BA, Dude A. The association between persistent maternal hypotension and small for gestational age neonates. Am J Obstet Gynecol MFM. 2021;3(6):100449. - PubMed
MeSH terms
Grants and funding
- Y2024012/Research Initiation Fund of Longgang District Maternity & Child Healthcare Hospital of Shenzhen City
- 81971417/National Natural Science Foundation of China
- LGKCYLWS2021000025/Medical and Health Science and Technology Plan attached to Longgang District Science and Technology Development Special Funding
- JCYJ20220530162415035/Shenzhen Municipal S&T programme
LinkOut - more resources
Full Text Sources
