

Ventilation distribution during spontaneous breathing trials predicts liberation from mechanical ventilation: the VISION study
- PMID: 39773268
- PMCID: PMC11705700
- DOI: 10.1186/s13054-024-05243-0
Ventilation distribution during spontaneous breathing trials predicts liberation from mechanical ventilation: the VISION study
Abstract
Background: Predicting complete liberation from mechanical ventilation (MV) is still challenging. Electrical impedance tomography (EIT) offers a non-invasive measure of regional ventilation distribution and could bring additional information.
Research question: Whether the display of regional ventilation distribution during a Spontaneous Breathing Trial (SBT) could help at predicting early and successful liberation from MV.
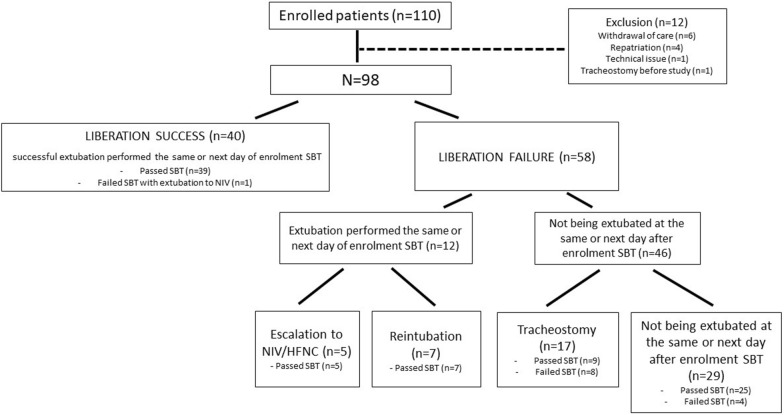
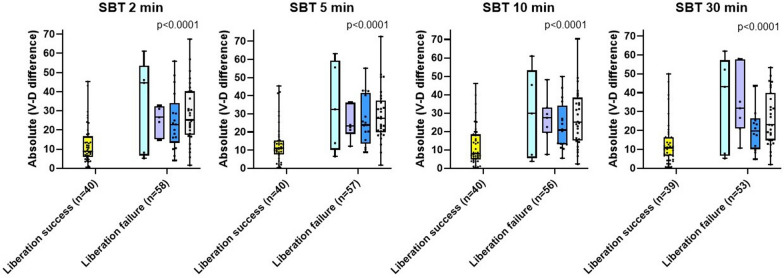
Study design and methods: Patients were monitored with EIT during the SBT. The tidal image was divided into ventral and dorsal regions and displayed simultaneously. We explored the ventral-to-dorsal ventilation difference in percentage, and its association with clinical outcomes. Liberation success was defined pragmatically as passing SBT followed by extubation within 24 h without reintubation for 7 days. Failure included use of rescue therapy, reintubation within 7 days, tracheostomy, and not being extubated within 24 h after succesful SBT. A training cohort was used for discovery, followed by a validation cohort.
Results: Among a total of 98 patients analyzed, 85 passed SBT (87%), but rapid liberation success occurred only in 40; 13.5% of extubated patients required reintubation. From the first minutes to the entire SBT duration, the absolute ventral-to-dorsal difference was consistently smaller in liberation success compared to all subgroups of failure (p < 0.0001). An absolute difference at 5 min of SBT > 20% was associated with failure of liberation, with sensitivity and specificity of 71% and 78% and positive predictive value 81% in a validation cohort.
Conclusion: During SBT, a large ventral-to-dorsal difference in ventilation indicated by EIT may help to rapidly identify patients at risk of liberation failure.
Keywords: Electrical impedance tomography; Ventilation-distribution; Weaning.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The Authors declare that they have no competing interest.
Figures


References
-
- Epstein SK, Ciubotaru RL. Independent effects of etiology of failure and time to reintubation on outcome for patients failing extubation. Am J Respir Crit Care Med. 1998;158(2):489–93. 10.1164/ajrccm.158.2.9711045. - PubMed
-
- Dres M, Younes M, Rittayamai N, et al. Sleep and pathological wakefulness at the time of liberation from mechanical ventilation (SLEEWE). A prospective multicenter physiological study. Am J Respir Crit Care Med. 2019;199(9):1106–15. 10.1164/rccm.201811-2119OC. - PubMed
-
- Pham T, Heunks L, Bellani G, et al. Weaning from mechanical ventilation in intensive care units across 50 countries (WEAN SAFE): a multicentre, prospective, observational cohort study. Lancet Respir Med. 2023;11(5):465–76. 10.1016/s2213-2600(22)00449-0. - PubMed
-
- Béduneau G, Pham T, Schortgen F, et al. Epidemiology of weaning outcome according to a new definition. The WIND study. Am J Respir Crit Care Med. 2017;195(6):772–83. 10.1164/rccm.201602-0320OC. - PubMed
-
- Peñuelas O, Frutos-Vivar F, Fernández C, et al. Characteristics and outcomes of ventilated patients according to time to liberation from mechanical ventilation. Am J Respir Crit Care Med. 2011;184(4):430–7. 10.1164/rccm.201011-1887OC. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
