

Intertransverse process block versus subcostal transversus abdominis plane block in patients undergoing laparoscopic radical gastrectomy: a prospective randomized controlled trial
- PMID: 39773318
- PMCID: PMC11706037
- DOI: 10.1186/s12871-024-02884-0
Intertransverse process block versus subcostal transversus abdominis plane block in patients undergoing laparoscopic radical gastrectomy: a prospective randomized controlled trial
Abstract
Background: Laparoscopic radical gastrectomy has been reported to be associated with substantial trauma and pain. This study compared the impact of ultrasound-(US)-guided, bilateral, double-injection intertransverse process block (ITPB) on postoperative analgesia with subcostal transversus abdominis plane block (TAPB) in patients who were undergoing laparoscopic radical gastrectomy.
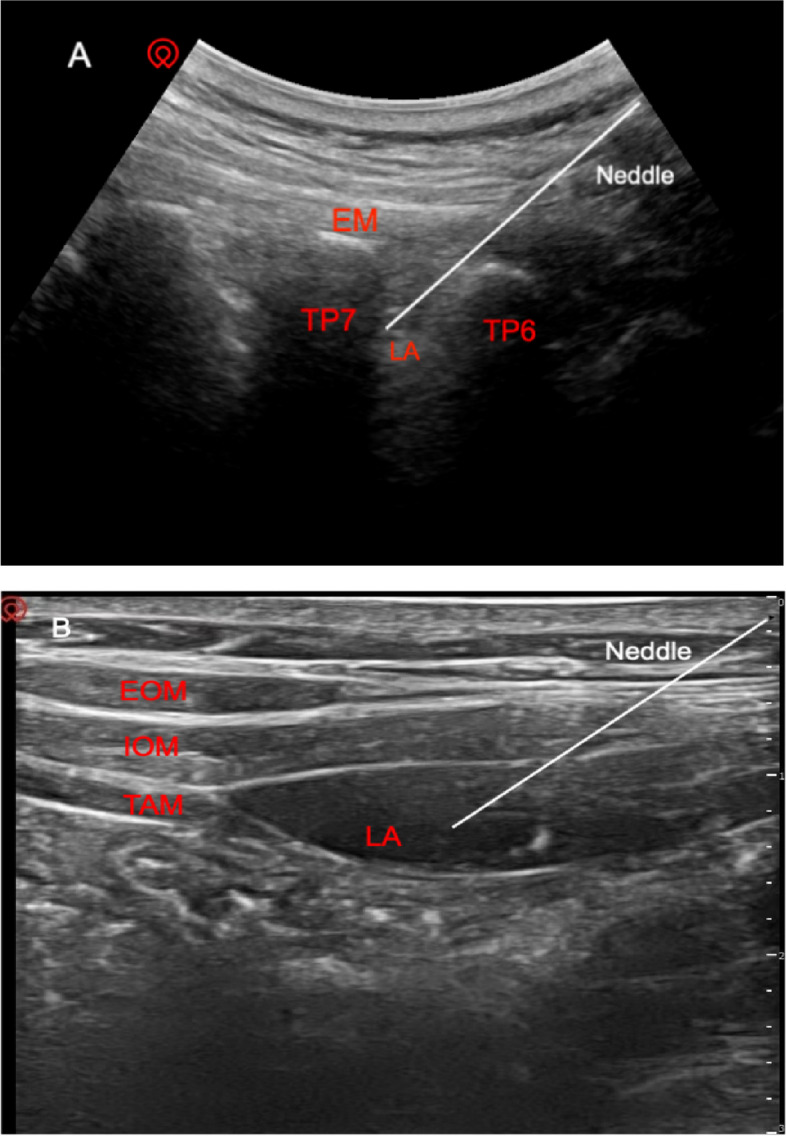
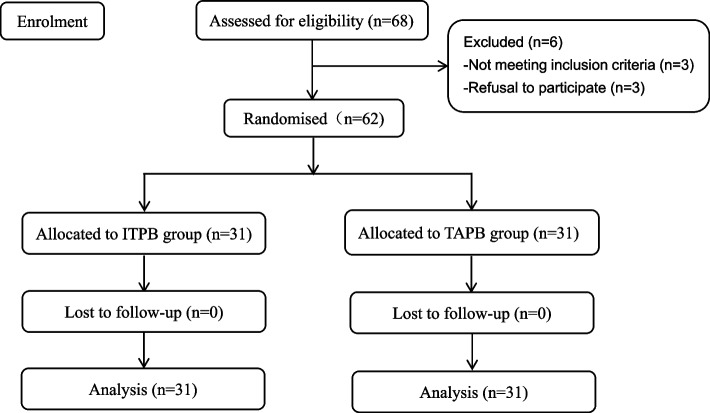
Methods: Sixty-two patients who were undergoing laparoscopic radical gastrectomy surgery under general anesthesia were included. These patients were randomized to either the ITPB group or the TAPB group. Patients in the ITPB group received a double-shot US-guided bilateral ITPB at the thoracic level T6/7 and T9/10 level using ropivacaine (0.3%, 15 mL). Patients in the TAPB group received bilateral subcostal TAPB one injection per side using ropivacaine (0.3%, 30 mL). All patients used a BIS-guided combined intravenous and inhalation anesthesia. The primary outcome was defined as postoperative morphine-equivalent consumption during the first 24 h.
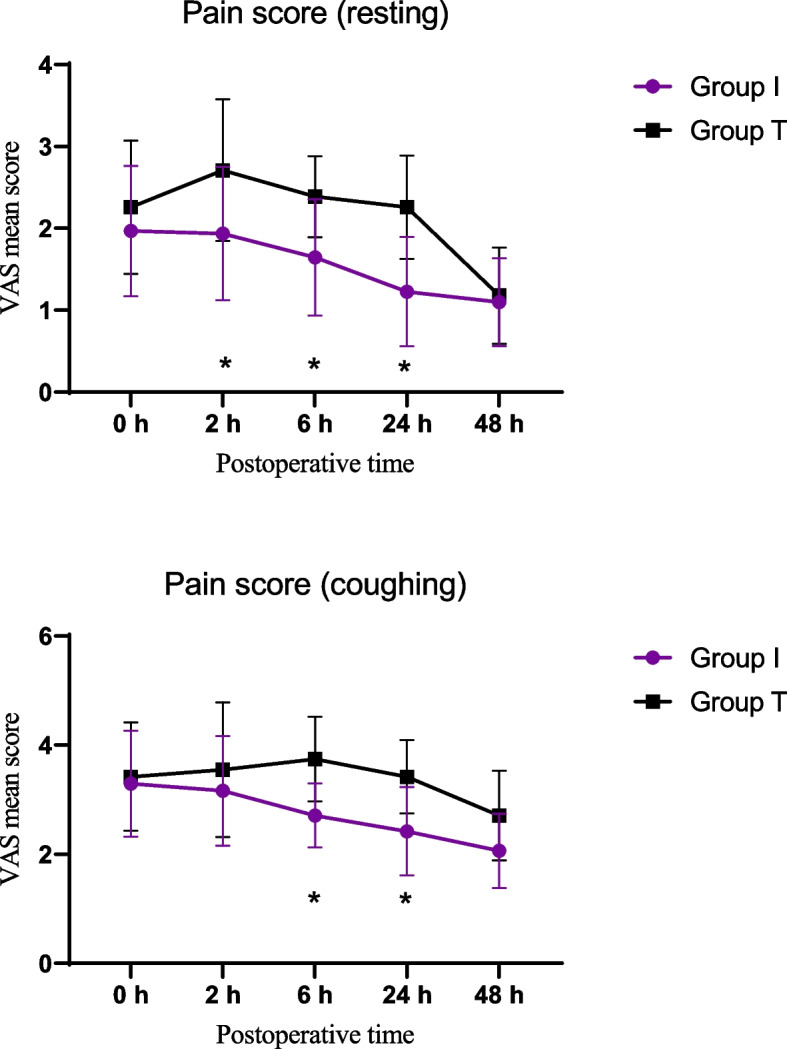
Results: The study recruited 62 patients (31 in each group) for the analysis. A comparatively less postoperative opioid consumption was observed in the ITPB group compared with the subcostal TAPB group within the first 24 h postoperatively (mean [standard deviation-(SD)] morphine-equivalent dose): 27.8 (5.7) mg vs 31.2 (4.4) mg, P < 0.001. The ITPB group showed lower intraoperative opioid use, and statistical significantly lower scores at rest and coughing at 6, 24 h postoperatively. The time to first requiring rescue analgesia was longer in the ITPB group than the subcostal TAPB group (median [IQR]): 8.0 [8.0] vs 6.0 [6.0] h, P = 0.009. The patients in the ITPB group exhibited earlier independent movement, lower incidence of postoperative complications and higher levels of satisfaction (P = 0.021).
Conclusion: This study showed that the double-shot bilateral ITPB could reduce opioids consumption and achieve longer and better pain relief. Additionally, it promoted early postoperative activity and improved patient satisfaction.
Trial registration: ChiCTR2300072986. Registered 29 June 2023.
Keywords: Intertransverse process block; Laparoscopic radical gastrectomy; Postoperative pain; Transversus abdominis plane block; Ultrasound-guided.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Ethics Committee of Yancheng First People's Hospital (2023-k-089, 17/06/2023). All patients provided signed informed consent forms. The trial registration number was as follows: ChiCTR2300072986, date of registration: 29/06/2023. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Effect of Subcostal Anterior Quadratus Lumborum Block vs. Oblique Subcostal Transversus Abdominis Plane Block after Laparoscopic Radical Gastrectomy.Curr Med Sci. 2021 Oct;41(5):974-980. doi: 10.1007/s11596-021-2429-8. Epub 2021 Sep 25. Curr Med Sci. 2021. PMID: 34562209
-
Erector spinae plane block versus transversus abdominis plane block with rectus sheath block for postoperative analgesia in laparoscopic hepatectomy: a randomized clinical trial.BMC Anesthesiol. 2025 Apr 9;25(1):162. doi: 10.1186/s12871-025-03031-z. BMC Anesthesiol. 2025. PMID: 40205560 Free PMC article. Clinical Trial.
-
The analgesic efficacy of subcostal transversus abdominis plane block compared with thoracic epidural analgesia and intravenous opioid analgesia after radical gastrectomy.Anesth Analg. 2013 Aug;117(2):507-13. doi: 10.1213/ANE.0b013e318297fcee. Epub 2013 Jun 6. Anesth Analg. 2013. PMID: 23744953 Clinical Trial.
-
Laparoscopic vs. ultrasound-guided transversus abdominis plane (TAP) block in colorectal surgery: a systematic review and meta-analysis of randomized trials.Surg Endosc. 2024 Mar;38(3):1119-1130. doi: 10.1007/s00464-023-10658-x. Epub 2024 Jan 22. Surg Endosc. 2024. PMID: 38253697
-
Postoperative Analgesia by a Transversus Abdominis Plane Block Using Different Concentrations of Ropivacaine for Abdominal Surgery: A Meta-Analysis.Clin J Pain. 2017 Sep;33(9):853-863. doi: 10.1097/AJP.0000000000000468. Clin J Pain. 2017. PMID: 28002093 Review.
References
-
- Yanagimoto Y, Takiguchi S, Miyazaki Y, et al. Comparison of pain management after laparoscopic distal gastrectomy with and without epidural analgesia. Surg Today. 2016;46(2):229–34. - PubMed
-
- You S, Xu F, Wu Y, et al. Effect of noise isolation using noise-cancelling headphones during laparoscopic surgery for postoperative pain reduction: a randomized clinical trial. J Clin Anesth. 2024;92:111286. - PubMed
-
- Kehlet H. Postoperative opioid sparing to hasten recovery: what are the issues?. Anesthesiology. 2005;102(6):1083–5. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
