

Effect of knee extension constraint training on walking biomechanics 6 months after anterior cruciate ligament reconstruction: a double-blind randomized controlled clinical trial
- PMID: 39773322
- PMCID: PMC11706006
- DOI: 10.1186/s13018-024-05447-8
Effect of knee extension constraint training on walking biomechanics 6 months after anterior cruciate ligament reconstruction: a double-blind randomized controlled clinical trial
Abstract
Background: The incidence of knee osteoarthritis after anterior cruciate ligament reconstruction (ACLR) is high to 57%, and the biomechanical abnormality during walking is one of the reasons. The purpose of this study was to investigate the effect of 12 weeks of knee extension constraint training on walking biomechanics during the stance phase of injured side after ACLR.
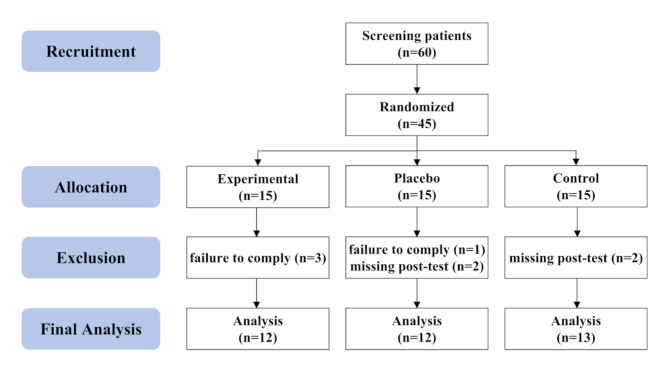
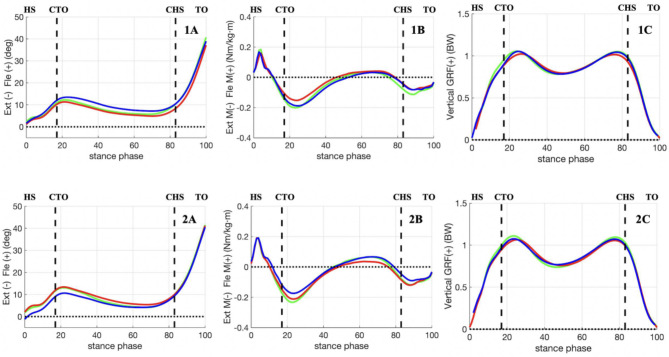
Methods: Forty-five patients were randomly assigned to three groups based on different brace conditions from 13 weeks to 24 weeks after ACLR: experimental (brace with knee extension constraint), placebo (brace without knee extension constraint), and control (no brace). Gait analysis was performed 3 and 6 months after ACLR. The peak for knee flexion angle (KFA), knee extension moment (KEM), and vertical ground reaction force (vGRF) were compared by 2 (time) x 3 (group) repeated-measures analysis of covariance (ANCOVA), and pairwise comparisons were conducted. .
Results: There was a significant time x group interaction for the peak KFA (p = 0.047), and there was no significant time x group interaction for the peak KEM and peak vGRF. The pairwise comparisons showed that there were no statistical differences among the groups both the pre-intervention and post-intervention in the peak KFA, peak KEM, and peak vGRF. Compared with pre-intervention, the peak vGRF in the experimental group was significantly greater (p = 0.009) and the peak KFA in the control group was significantly lower (p = 0.041) post-intervention. There were not significantly different in the placebo group between pre-intervention and post-intervention.
Conclusion: 12 weeks of knee extension constraint training can increase lower extremity loading on the injured side, may be a potential therapeutic adjunct to improve abnormal gait after ACLR.
Keywords: Anterior cruciate ligament reconstruction; Biomechanics; Rehabilitation; Walking.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: Ethics approval was obtained from Peking University Third Hospital Medical Science Research Ethics Committee (IRB00006761-2015243). Consent to participate: Informed consent was obtained from all individual participants included in the study. Consent for publication: All authors have approved the release of their work to the public. Competing interests: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Musahl V, Karlsson J. Anterior cruciate ligament tear. N Engl J Med. 2019;380(24):2341–8. - PubMed
-
- Mall NA, Chalmers PN, Moric M, Tanaka MJ, Cole BJ, Bach BR Jr., Paletta GA. Jr. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42(10):2363–70. - PubMed
-
- Skvortsov D, Kaurkin S, Goncharov E, Akhpashev A. Knee joint function and walking biomechanics in patients in acute phase anterior cruciate ligament tear. Int Orthop. 2020;44(5):885–91. - PubMed
-
- Barenius B, Ponzer S, Shalabi A, Bujak R, Norlen L, Eriksson K. Increased risk of osteoarthritis after anterior cruciate ligament reconstruction: a 14-year follow-up study of a randomized controlled trial. Am J Sports Med. 2014;42(5):1049–57. - PubMed
-
- Pietrosimone B, Blackburn JT, Padua DA, Pfeiffer SJ, Davis HC, Luc-Harkey BA, Harkey MS, Stanley Pietrosimone L, Frank BS, Creighton RA, Kamath GM, Spang JT. Walking gait asymmetries 6 months following anterior cruciate ligament reconstruction predict 12-month patient-reported outcomes. J Orthop Res. 2018;36(11):2932–40. - PubMed
Publication types
MeSH terms
Grants and funding
- 2022SKY363/Tianjin Research Innovation Project for Postgraduate Students
- 20230484412/Beijing Nova Program
- L222138/Beijing Natural Science Foundation
- BYSYZHKC2022119/Innovation and Transformation Fund Project of Peking University Third Hospital
- BYSYZD2021012/Clinical Key Projects of Peking University Third Hospital
LinkOut - more resources
Full Text Sources
Medical
