

Can home care work be organized to promote musculoskeletal health for workers? Results from the GoldiCare cluster randomized controlled trial
- PMID: 39773460
- PMCID: PMC11708094
- DOI: 10.1186/s12913-024-12133-2
Can home care work be organized to promote musculoskeletal health for workers? Results from the GoldiCare cluster randomized controlled trial
Abstract
Background: Workers in home care have high sick leave rates, predominantly because of musculoskeletal pain. The Goldilocks Work Principle proposes that health should be promoted by a "just right" composition of work tasks. Weekly workloads differ substantially between home care workers, suggesting that certain workers may have workloads that are too high, impacting their musculoskeletal health. The aim of this study was to evaluate the effectiveness of a "GoldiCare" intervention redistributing weekly workloads to become more equal among the homecare workers. Outcomes were pain in the neck/shoulder and lower back, and the implementation of the intervention was also evaluated.
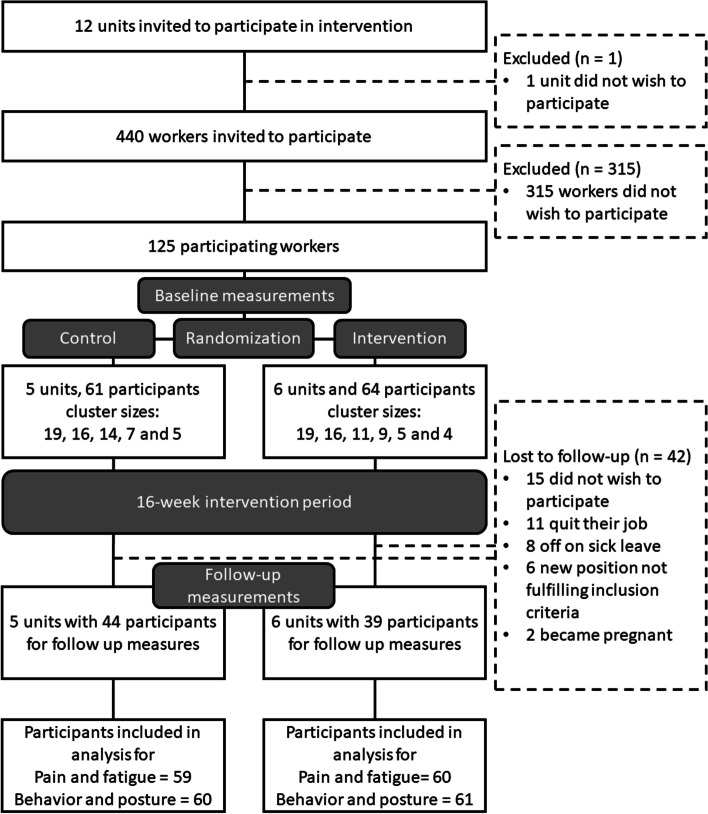
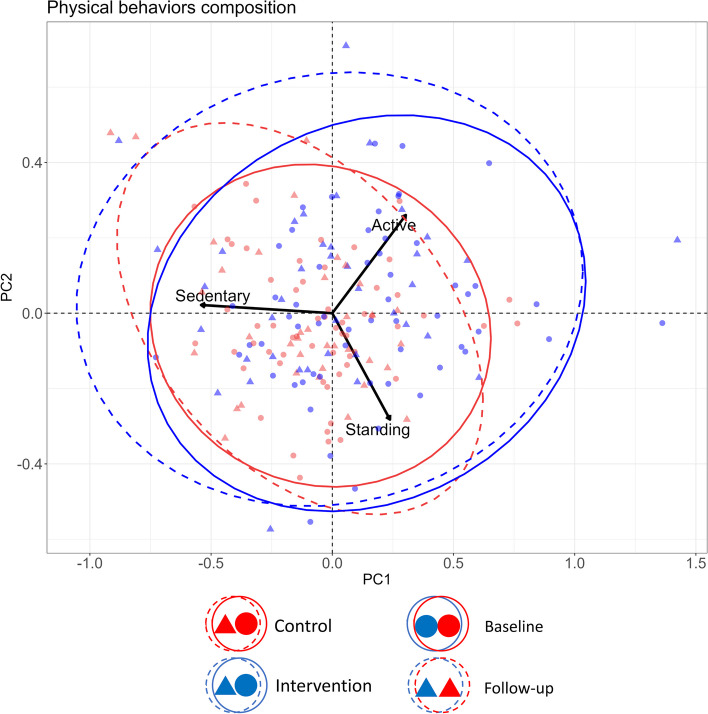
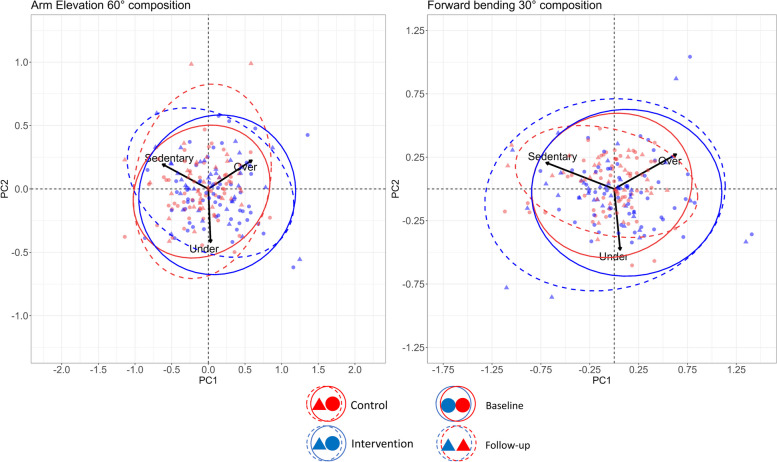
Methods: A 16-week cluster randomized controlled trial was conducted with 125 workers from 11 home care units, divided into six intervention units and five control units. The operation coordinators of each intervention unit were educated in the Goldilocks Work Principle and provided with a planning tool to facilitate an even distribution of high care need clients. The control group continued their usual work. Primary outcomes were pain intensity in the neck/shoulder and lower back (0 to 10). Secondary outcomes included fatigue (0 to 10), composition of physical behaviors and postures (accelerometers), adherence to the intervention (weekly usage rates of the planning tool), and performance of the intervention (percentage of workers with an even distribution of workload).
Results: The analysis showed no difference between the intervention and control groups in change in lower back pain (0.07, 95%CI[-0.29;0.43]), neck/shoulder pain (-0.06, 95%CI[-0.49;0.36]) or fatigue (0.04, 95%CI[-0.52;0.61]. No significant changes were observed in the composition of physical behaviors (p = 0.067) or postures (p = 0.080-0.131) between the two groups. The intervention was succesfully implemented in three units of the six, with adherence ranging from 82-100% across the intervention period. The remaining three units had an adherence of 0-47%. No improvement in performance was observed.
Conclusion: No significant intervention effects were observed on musculoskeletal pain, fatigue, or the composition of physical behaviors and postures. The findings suggest that the intervention was not adequately implemented within the organization. Consequently, we cannot discern whether the lack of positive results were due to poor implementation or an ineffective intervention. Results thus highlight the need for a more comprehensive understanding of organizational structures within home care to facilitate more effective implementations. The hypothetical effectiveness of a fully implemented intervention remains unknown.
Trial registration: Clinicaltrials.gov ID: NCT05487027, submitted: 03/08/2022.
Keywords: Clinical trial; Cluster randomized controlled trial; Compositional analysis; Goldilocks work; Home care; Norway; Worker health.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Regional Committee for Medical Research Ethics Central Norway (REK central) approved of this study (#315556). All home care workers who participated in the measurements signed an informed consent sheet informing them of their rights in accordance with the Helsinki Declaration. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- Helsedirektoratet. Kommunale helse- og omsorgstjenester 2022: Helsedirektoratet; 2023. Available from: https://www.helsedirektoratet.no/rapporter/kommunale-helse-og-omsorgstje....
-
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2022: Summary of Results. 2022;UN DESA/POP/2022/TR/NO. 3.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
