

Cohort profile: creation of the SAIL MELD-B e-cohort (SMC) and SAIL MELD-B children and young adult e-cohort (SMYC) to investigate the lived experience of the 'burdensomeness' of multimorbidity
- PMID: 39773797
- PMCID: PMC11792564
- DOI: 10.1136/bmjopen-2024-087946
Cohort profile: creation of the SAIL MELD-B e-cohort (SMC) and SAIL MELD-B children and young adult e-cohort (SMYC) to investigate the lived experience of the 'burdensomeness' of multimorbidity
Abstract
Purpose: We have established the SAIL MELD-B electronic cohort (e-cohort SMC) and the SAIL MELD-B children and Young adults e-cohort (SMYC) as a part of the Multidisciplinary Ecosystem to study Lifecourse Determinants and Prevention of Early-onset Burdensome Multimorbidity (MELD-B) project. Each cohort has been created to investigate and develop a deeper understanding of the lived experience of the 'burdensomeness' of multimorbidity by identifying new clusters of burdensomeness concepts, exploring early life risk factors of multimorbidity and modelling hypothetical prevention scenarios.
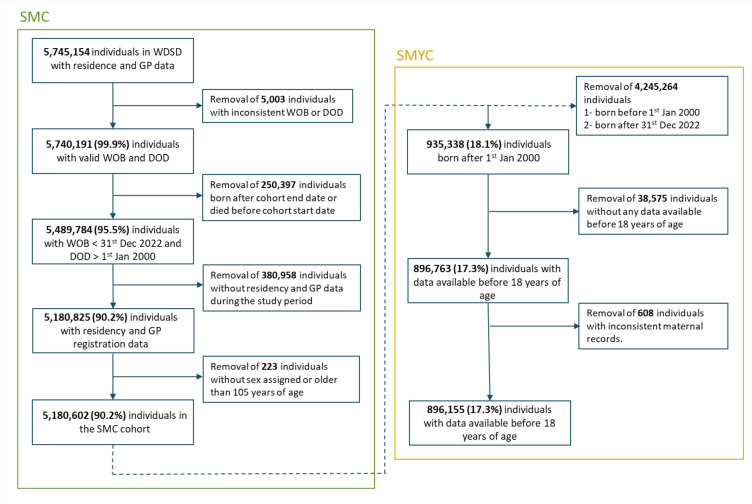
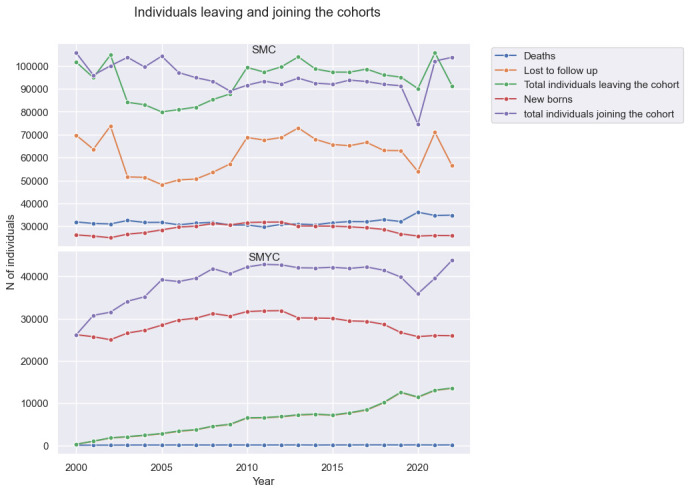
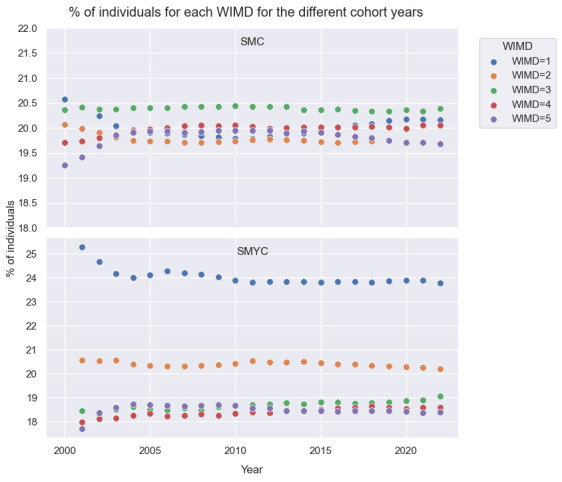
Participants: The SMC and SMYC are longitudinal e-cohorts created from routinely collected individual-level population-scale anonymised data sources available within the Secure Anonymised Information Linkage (SAIL) Databank. They include individuals with available records from linked health and demographic data sources in SAIL at any time between 1 January 2000 and 31 December 2022. The SMYC e-cohort is a subset of the SMC, including only individuals born on or after the cohort start date.
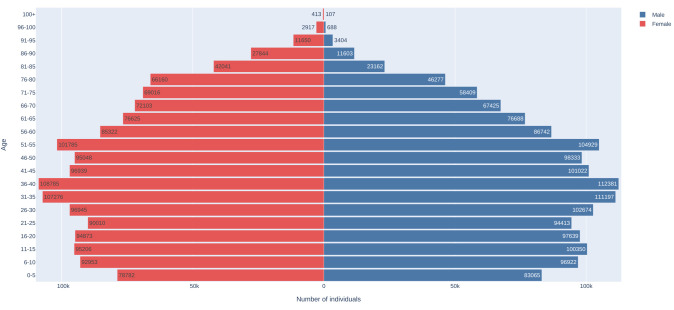
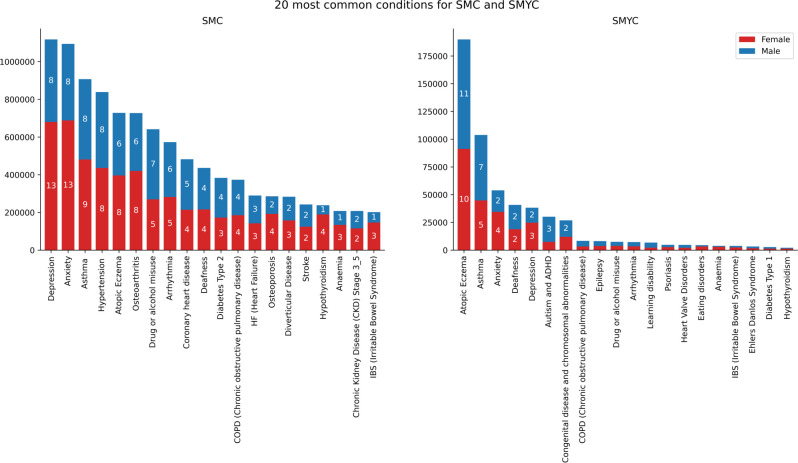
Findings to date: The SMC and SMYC cohorts include 5 180 602 (50.3% female and 49.7% male) and 896 155 (48.7% female and 51.3% male) individuals, respectively. Considering both primary and secondary care health data, the five most common long-term conditions for individuals in SMC are 'Depression', affecting 21.6% of the cohort, 'Anxiety' (21.1%), 'Asthma' (17.5%), 'Hypertension' (16.2%) and 'Atopic Eczema' (14.1%) and the five most common conditions for individuals in SMYC are 'Atopic Eczema' (21.2%), 'Asthma' (11.6%), 'Anxiety' (6.0%), 'Deafness' (4.6%) and 'Depression' (4.3%).
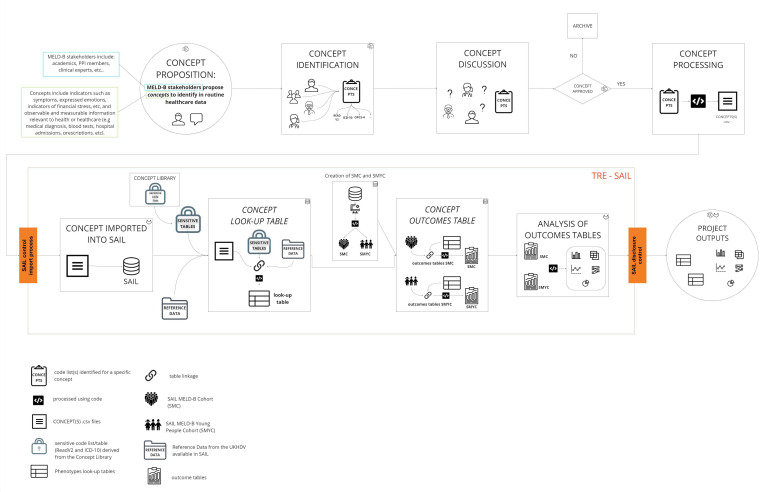
Future plans: The SMC and SMYC e-cohorts have been developed using a reproducible, maintainable concept curation pipeline, which allows for the cohorts to be updated dynamically over time and manages for the request and processing of further approved long-term conditions and burdensomeness concepts extraction. Best practices from the MELD-B project can be utilised across other projects, accessing similar data with population-scale data sources and trusted research environments.
Keywords: Chronic Disease; Electronic Health Records; Multimorbidity; STATISTICS & RESEARCH METHODS.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY. Published by BMJ Group.
Conflict of interest statement
Competing interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: RKO is a member of the National Institute for Health and Care Excellence (NICE) Technology Appraisal Committee, member of the NICE Decision Support Unit (DSU)and associate member of the NICE Technical Support Unit (TSU). She has served as a paid consultant providing unrelated methodological advice to AstraZeneca, Cogentia Healthcare Ltd, Daiichi Sankyo, NICE, the Norwegian Institute of Public Health, Roche and Vifor Pharma. She reports teaching fees from the Association of British Pharmaceutical Industry (ABPI) and the University of Bristol. RH is a member of the Scientific Board of the Smith Institute for Industrial Mathematics and System Engineering. All other authors declare that there are no further conflicts of interest.
Figures
Similar articles
-
Associations between multimorbidity and adverse health outcomes in UK Biobank and the SAIL Databank: A comparison of longitudinal cohort studies.PLoS Med. 2022 Mar 7;19(3):e1003931. doi: 10.1371/journal.pmed.1003931. eCollection 2022 Mar. PLoS Med. 2022. PMID: 35255092 Free PMC article.
-
Multidisciplinary ecosystem to study lifecourse determinants and prevention of early-onset burdensome multimorbidity (MELD-B) - protocol for a research collaboration.J Multimorb Comorb. 2023 Sep 25;13:26335565231204544. doi: 10.1177/26335565231204544. eCollection 2023 Jan-Dec. J Multimorb Comorb. 2023. PMID: 37766757 Free PMC article.
-
Protocol for the development of the Wales Multimorbidity e-Cohort (WMC): data sources and methods to construct a population-based research platform to investigate multimorbidity.BMJ Open. 2021 Jan 19;11(1):e047101. doi: 10.1136/bmjopen-2020-047101. BMJ Open. 2021. PMID: 33468531 Free PMC article.
-
Changes in Depression and Anxiety Among Children and Adolescents From Before to During the COVID-19 Pandemic: A Systematic Review and Meta-analysis.JAMA Pediatr. 2023 Jun 1;177(6):567-581. doi: 10.1001/jamapediatrics.2023.0846. JAMA Pediatr. 2023. PMID: 37126337 Free PMC article.
-
Use of public datasets in the examination of multimorbidity: Opportunities and challenges.Mech Ageing Dev. 2020 Sep;190:111310. doi: 10.1016/j.mad.2020.111310. Epub 2020 Jul 2. Mech Ageing Dev. 2020. PMID: 32622995 Review.
Cited by
-
Capturing the human impact of living with multiple long-term conditions in routine electronic health records - lost in translation?J Multimorb Comorb. 2025 Apr 1;15:26335565251329869. doi: 10.1177/26335565251329869. eCollection 2025 Jan-Dec. J Multimorb Comorb. 2025. PMID: 40176980 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources