

Is longer really better? Results of a retrospective real-life cohort study evaluating the benefit of adding a weekly educational session to a traditional 8-week home-based pulmonary rehabilitation programme in people with COPD
- PMID: 39773805
- PMCID: PMC11749871
- DOI: 10.1136/bmjopen-2024-092096
Is longer really better? Results of a retrospective real-life cohort study evaluating the benefit of adding a weekly educational session to a traditional 8-week home-based pulmonary rehabilitation programme in people with COPD
Abstract
Objectives: To evaluate the short-term and long-term benefits of adding a weekly educational session to a traditional 8-week home-based pulmonary rehabilitation (PR) programme in people with chronic obstructive pulmonary disease (COPD). Primary hypothesis was that 8 home-based supervised sessions will be equivalent to 16 home-based supervised sessions at both short- and long-term after PR.
Design: Retrospective cohort study conducted on prospectively collected real-life data, from January 2010 to December 2021.
Setting: FormAction Santé, Pérenchies France.
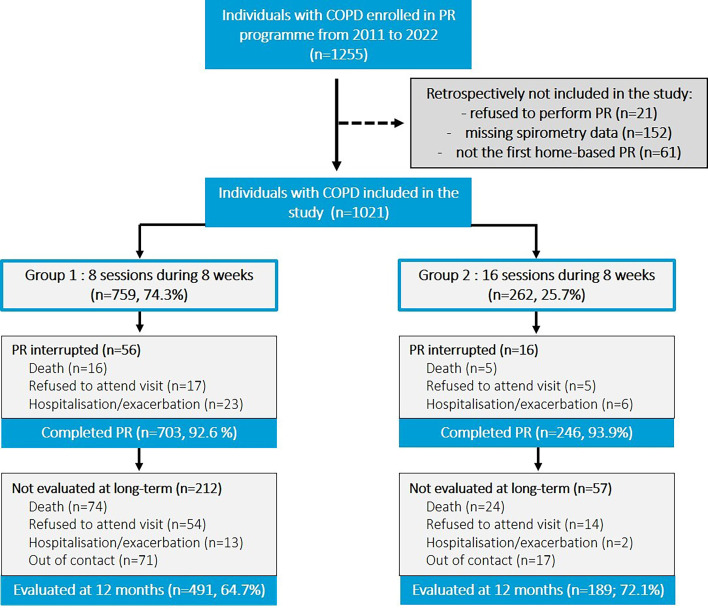
Participants: Eligible individuals were aged >18 years with a diagnosis of COPD and referred to the home-based PR programme by their respiratory physician. Participants were retrospectively divided into two groups (Gr 1, 8 PR sessions, n=759, and Gr 2, 8 PR sessions+8 educational sessions, n=262).
Intervention: All participants received an 8-week personalised home PR programme. A subgroup of participants received one additional supervised home session per week, including education and motivational support for daily physical activities and walking.
Outcomes: Health-related quality of life, dyspnoea, anxiety and depressive symptoms, fatigue and exercise tolerance were assessed at baseline (M0), at the end of PR (M2), and 14 months (M14) after M0.
Results: Baseline characteristics and assessments were similar between groups with an exception for long-term oxygen therapy (Gr1: 69.8% vs Gr2 53.0%, p<0.001) and noninvasive ventilation (Gr1: 38.6% vs Gr2: 29.8%, p=0.015). At M2 and M14, all the assessments were improved in both groups (p<0.01). At M2, the improvement in health status and exercise tolerance was higher in Gr 2 compared with Gr 1 (p<0.05). From M0 to M14, 90 (11.9%) participants and 29 (11.1%) participants died in Gr 1 and Gr 2, respectively (p=0.794).
Conclusion: People with COPD benefited, at short and long terms, from both 8 or 16 supervised home-based PR sessions. Once-weekly home-based supervised sessions during 8 weeks, combined with unsupervised physical training sessions and self-management plan for the other health behaviours, might be the best compromise between patients, health professionals and policy makers.
Keywords: Health Education; Pulmonary Disease, Chronic Obstructive; REHABILITATION MEDICINE.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: OLR reports personal fees and non-financial support unrelated to the submitted work from AstraZeneca, Boehringer Ingelheim, Chiesi, CSL Behring, GlaxoSmithKline, MSD France, Vertex and Vitalaire. OLR is principal investigator in studies for Vertex and CSL Behring. SP is employed by Santélys company. CC reports personal fees and non-financial support unrelated to the submitted work from ALK-Abello, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKlein, MEDA Pharma, Medexact, Novartis, Pierre Fabre, Pfizer, Roche, Sanofi, Santélys, and TEVA. JMG reports personal fees and non-financial support unrelated to the submitted work from AstraZeneca, Boehringer Ingelheim, Chiesi, CSL Behring, GlaxoSmithKlein.
Figures

Similar articles
-
Physical and affective components of dyspnoea are improved by pulmonary rehabilitation in COPD.BMJ Open Respir Res. 2022 Jan;9(1):e001160. doi: 10.1136/bmjresp-2021-001160. BMJ Open Respir Res. 2022. PMID: 35078826 Free PMC article.
-
A randomized controlled trial of telephone-mentoring with home-based walking preceding rehabilitation in COPD.Int J Chron Obstruct Pulmon Dis. 2016 Aug 25;11:1991-2000. doi: 10.2147/COPD.S109820. eCollection 2016. Int J Chron Obstruct Pulmon Dis. 2016. PMID: 27601892 Free PMC article. Clinical Trial.
-
Comparison of unsupervised home-based pulmonary rehabilitation versus supervised hospital outpatient pulmonary rehabilitation in patients with chronic obstructive pulmonary disease.Expert Rev Respir Med. 2019 Dec;13(12):1195-1203. doi: 10.1080/17476348.2019.1675516. Epub 2019 Oct 9. Expert Rev Respir Med. 2019. PMID: 31575305
-
Active mind-body movement therapies as an adjunct to or in comparison with pulmonary rehabilitation for people with chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2018 Oct 10;10(10):CD012290. doi: 10.1002/14651858.CD012290.pub2. Cochrane Database Syst Rev. 2018. PMID: 30306545 Free PMC article.
-
Psychological therapies for the treatment of depression in chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2019 Mar 6;3(3):CD012347. doi: 10.1002/14651858.CD012347.pub2. Cochrane Database Syst Rev. 2019. PMID: 30838649 Free PMC article.
References
-
- Société de Pneumologie de Langue Française (SPLF) Réhabilitation du patient atteint de BPCO. Rev Mal Respir. 2010;27:S36–69. doi: 10.1016/S0761-8425(10)70005-X. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials