

Use of virtual care near the end of life before and during the COVID-19 pandemic: A population-based cohort study
- PMID: 39774523
- PMCID: PMC11709317
- DOI: 10.1371/journal.pone.0313766
Use of virtual care near the end of life before and during the COVID-19 pandemic: A population-based cohort study
Abstract
Background and aims: The expanded use of virtual care may worsen pre-existing disparities in use and delivery of end-of-life care among certain groups of people. We measured the use of virtual care in the last three months of life before and after the introduction of virtual care fee codes that funded care delivery at the start of COVID-19 on March 14, 2020, and identified changes in the characteristics of people using it.
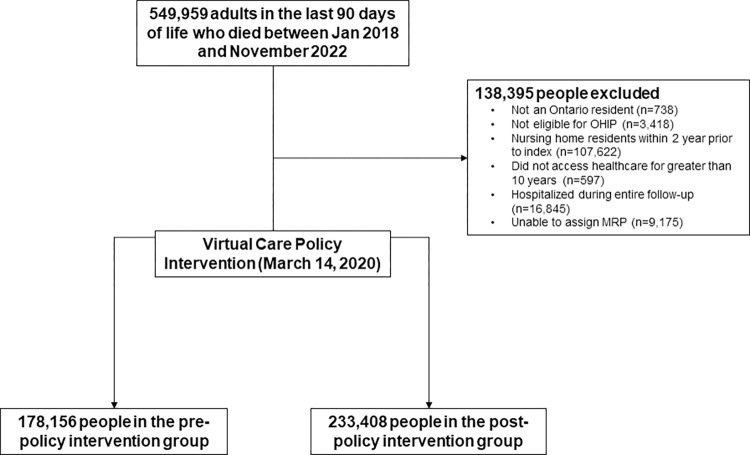
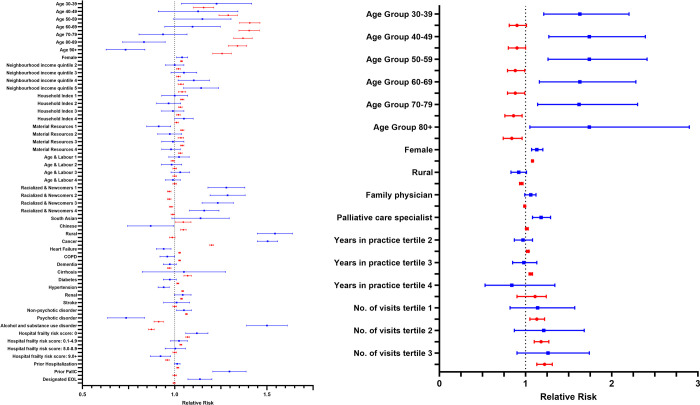
Methods: We used linked clinical and administrative datasets to study use of virtual care in the last three months of life among 411,564 adults who died between January 25, 2018, and November 30, 2022. Modified Poisson regression was used to measure the association of the use of virtual care in the last three months of life with the pandemic study period and its association with each person- and physician-level factor.
Results: 14,261 people (8%) used virtual care in the last three months of life before the pandemic, and 161,000 people (69%) used it during the pandemic (relative risk [RR] 8.76; 95% CI 8.48-9.05). Several individual patient characteristics were associated with statistically significant increases in the use of virtual care after March 14, 2020 (following the introduction of virtual care fee codes), compared to before such as among older adults, ethnic minorities, multiple chronic comorbid health conditions and higher frailty groups.
Conclusions: The introduction of new fee codes broadening technology and funding for end-of-life care at the start of pandemic combined with pandemic-related effects was associated with a substantial increase in the use of virtual care near the end of life among certain groups and a general leveling of pre-existing disparities in its use. Virtual end-of-life care delivery may strengthen person-centredness for individuals with limited ability to attend in-person appointments and by providers who may not have previously engaged in such care.
Copyright: © 2025 Quinn et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Comparison of physician-delivered models of virtual and home-based in-person care for adults in the last 90 days of life with cancer and terminal noncancer illness during the COVID-19 pandemic.PLoS One. 2024 Nov 27;19(11):e0301813. doi: 10.1371/journal.pone.0301813. eCollection 2024. PLoS One. 2024. PMID: 39602394 Free PMC article.
-
Association of physician-delivered virtual care near the end of life with healthcare use outcomes: A national population-based study of Canadians.PLoS One. 2025 Jun 3;20(6):e0324898. doi: 10.1371/journal.pone.0324898. eCollection 2025. PLoS One. 2025. PMID: 40460327 Free PMC article.
-
Using Administrative Data to Explore Potentially Aberrant Provision of Virtual Care During COVID-19: Retrospective Cohort Study of Ontario Provincial Data.J Med Internet Res. 2021 Sep 7;23(9):e29396. doi: 10.2196/29396. J Med Internet Res. 2021. PMID: 34313590 Free PMC article.
-
Growing inequities by immigration group among older adults: population-based analysis of access to primary care and return to in-person visits during the COVID-19 pandemic in British Columbia, Canada.BMC Prim Care. 2024 Sep 6;25(1):332. doi: 10.1186/s12875-024-02530-1. BMC Prim Care. 2024. PMID: 39243016 Free PMC article.
-
Antibiotic Prescribing by Digital Health Care Providers as Compared to Traditional Primary Health Care Providers: Cohort Study Using Register Data.J Med Internet Res. 2024 Jun 26;26:e55228. doi: 10.2196/55228. J Med Internet Res. 2024. PMID: 38924783 Free PMC article.
References
-
- Association Canadian Medical. Virtual Care in Canada. 2019. https://www.cma.ca/sites/default/files/pdf/News/Virtual_Care_discussionp....
-
- Beresford L. Is Telemedicine the Future of Palliative Care? 2020; published online Sept 3. https://www.medpagetoday.com/practicemanagement/telehealth/88448 (accessed 1AD).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
