

Pediatric Mycosis Fungoides Mimicking Benign Dermatoses: A Report of a Rare Case
- PMID: 39774580
- PMCID: PMC11725661
- DOI: 10.12659/AJCR.945897
Pediatric Mycosis Fungoides Mimicking Benign Dermatoses: A Report of a Rare Case
Abstract
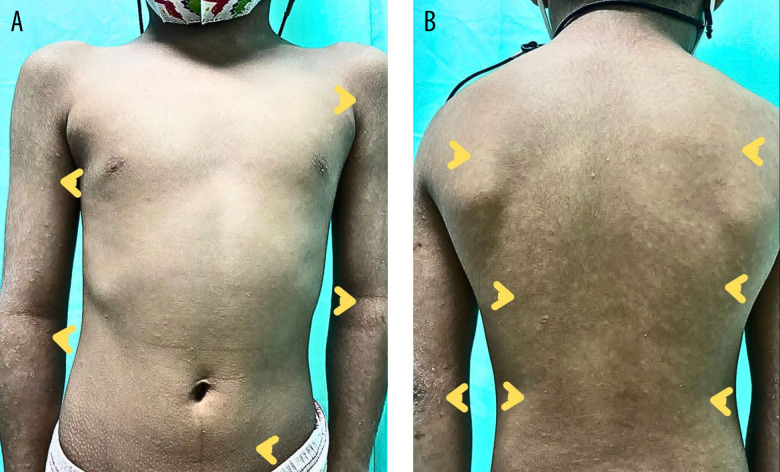
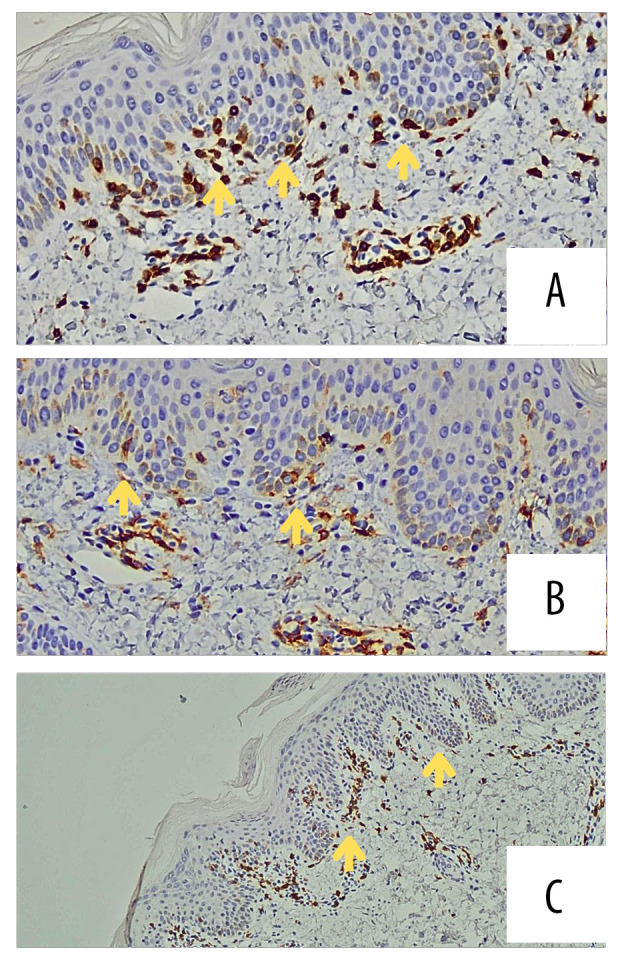
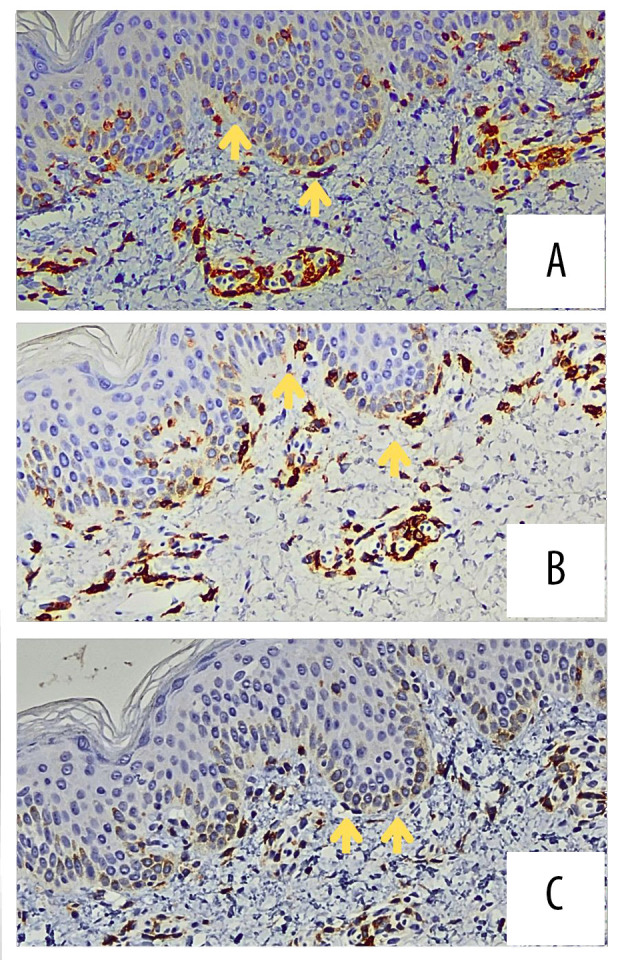
BACKGROUND Primary cutaneous lymphomas (PCL) are a multifaceted spectrum of cutaneous T cell lymphoma (CTCL) and cutaneous B cell lymphomas (CBCL). Mycosis fungoides (MF) is a rare subset of CTCL that primarily affects adults, and its occurrence in children is exceedingly rare. Most pediatric MF manifests as hypopigmented patches resembling other benign dermatoses, causing diagnostic challenges. This report outlines a case of pediatric MF in a 7-year-old Malaysian boy. CASE REPORT A 7-year-old boy exhibited progressing skin lesions characterized initially by erythematous, papular rashes over the face and upper limbs, then to the whole body, becoming hypopigmented, with pruritus and scaling for 1 year. Multiple clinics treated him for eczema and pityriasis alba but he responded poorly to courses of various topical steroids and emollient treatment. Due to the refractory nature of the lesions, he was subsequently referred to a dermatology clinic, where 2 skin biopsies were performed. The first biopsy revealed epidermotropism of atypical lymphocytes, consistent with MF. Immunohistochemical analysis revealed positive CD3+ expression with slightly reduced CD4+, CD7+, and CD8+ expression, and normal CD2+ and CD5+ expression at the epidermis level. Nevertheless, due to the rarity of MF in children, a second biopsy was performed, validating the diagnosis. CONCLUSIONS Pediatric MF is a rare and challenging diagnosis. This case report highlights the importance of close monitoring of unresolved hypopigmented lesions and increased vigilance on lesions not responding to standard treatment. Timely diagnosis with support of skin biopsy is crucial to avoid potentially serious disease progression and helps provide appropriate management leading to improved outcomes.
Conflict of interest statement
Figures



Similar articles
-
Pityriasis Lichenoid-like Mycosis Fungoides in a 9-year-old Boy: A Case Report.Acta Dermatovenerol Croat. 2019 Mar;27(1):37-39. Acta Dermatovenerol Croat. 2019. PMID: 31032790
-
Mycosis fungoides with spongiosis: a case report.J Med Case Rep. 2023 Nov 3;17(1):458. doi: 10.1186/s13256-023-04188-2. J Med Case Rep. 2023. PMID: 37919795 Free PMC article.
-
Childhood hypopigmented mycosis fungoides: a commonly delayed diagnosis.BMJ Case Rep. 2014 Dec 23;2014:bcr2014208306. doi: 10.1136/bcr-2014-208306. BMJ Case Rep. 2014. PMID: 25538219 Free PMC article.
-
Primary cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome): part I. Diagnosis: clinical and histopathologic features and new molecular and biologic markers.J Am Acad Dermatol. 2014 Feb;70(2):205.e1-16; quiz 221-2. doi: 10.1016/j.jaad.2013.07.049. J Am Acad Dermatol. 2014. PMID: 24438969 Review.
-
[Papular mycosis fungoides].Ann Dermatol Venereol. 2013 Jun-Jul;140(6-7):455-8. doi: 10.1016/j.annder.2013.04.072. Epub 2013 May 22. Ann Dermatol Venereol. 2013. PMID: 23773745 Review. French.
References
-
- Groves FD, Linet MS, Travis LB, Devesa SS. Cancer surveillance series: Non-Hodgkin’s lymphoma incidence by histologic subtype in the United States from 1978 through 1995. J Natl Cancer Inst. 2000;92(15):1240–51. - PubMed
-
- Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768–85. - PubMed
-
- Ferenczi K, Makkar HS. Cutaneous lymphoma: Kids are not just little people. Clin Dermatol. 2016;34(6):749–59. - PubMed
-
- Yazganoglu KD, Topkarci Z, Buyukbabani N, Baykal C. Childhood mycosis fungoides: A report of 20 cases from Turkey. J Eur Acad Dermatology Venereol. 2013;27(3):295–300. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
