

Forearm elevation impairs local static handgrip endurance likely through reduction in vascular conductance and perfusion pressure: revisiting Rohmert's curve
- PMID: 39774653
- PMCID: PMC11707015
- DOI: 10.1038/s41598-024-83939-7
Forearm elevation impairs local static handgrip endurance likely through reduction in vascular conductance and perfusion pressure: revisiting Rohmert's curve
Abstract
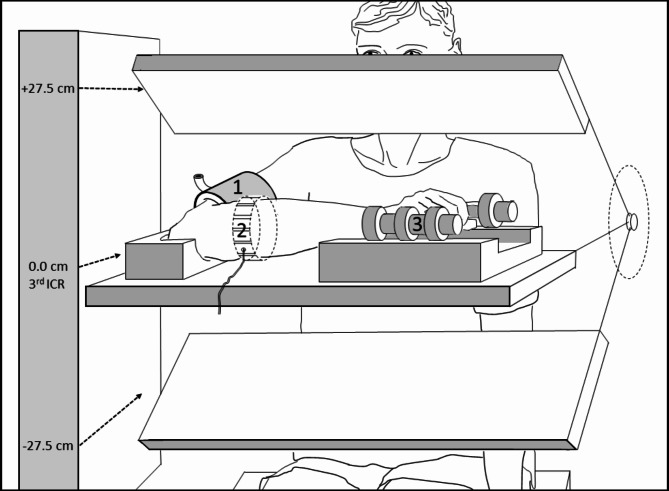
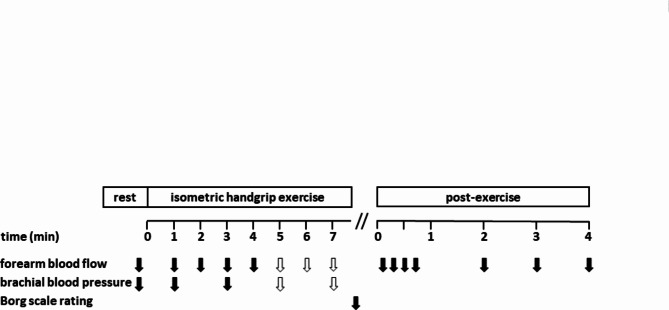
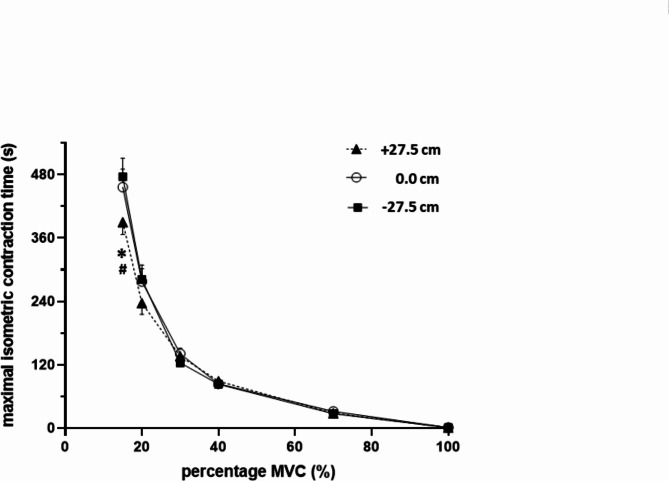
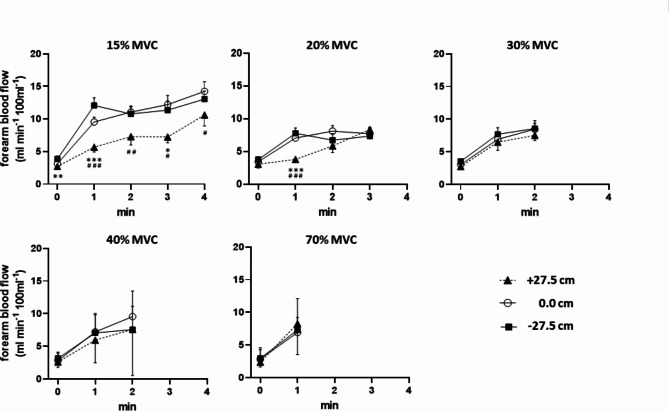
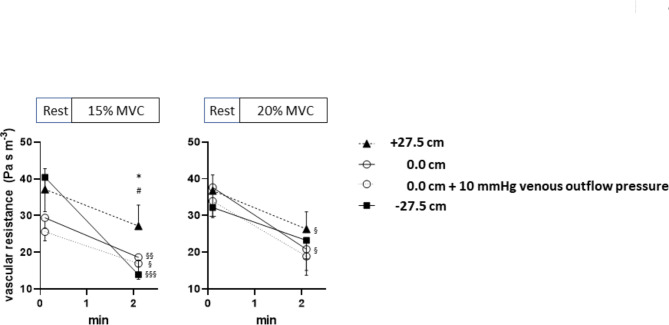
Maximal isometric contraction time (MICT) is critical for most motor tasks and depends on skeletal muscle blood flow at < 40% of maximal voluntary strength (MVC). Whether limb work positions associated with reduced perfusion pressure and facilitated vessel compression affect MICT is largely unknown. In 14 healthy young men we therefore assessed bilateral handgrip MICT at 15, 20, 30, 40, and 70% of MVC in horizontal forearm positions of 0.0, + 27.5 or - 27.5 cm relative to heart level. Forearm blood flow (FBF, venous occlusion plethysmography) and brachial blood pressure were measured repetitively. MICT at 15% MVC was significantly shorter by 66.3 and 86.2 s with forearm position + 27.5 cm (389.6 ± 23.3 s) as compared to 0.0 cm (455.9 ± 34.1 s) and - 27.5 cm (475.8 ± 35.0 s) while MICT at 20-70% MVC was unaffected. Peak FBF at 15% MVC was significantly lower in position + 27.5 cm (11.11 ± 0.92 ml/min/100 ml) compared to 0.0 cm (15.55 ± 0.91 ml/min/100 ml) or - 27.5 cm (14.21 ± 0.59 ml/min/100 ml) and vascular resistance significantly higher in position + 27.5 vs 0.0 or - 27.5 cm. Working position above, but not below heart level may limit MICT at 15% MVC possibly through blood flow reduction arising from increased vascular resistance beside reduced perfusion pressure. Local isometric endurance warrants (re)evaluation regarding hydrostatic/gravitational or other hemodynamic limitations.
Keywords: Blood flow; Fatigue; Gravitation; Hydrostatic pressure; Skeletal muscle; Static exercise.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Data availability: The data sets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Figures
References
-
- Rohmert, W. Die Grundlage der Beurteilung statischer Arbeit (Westdeutscher Verlag ISSN 0367-3421, 1960).
-
- Kilbom, A. Circulatory adaptation during static muscular contractions. A review. Scand. J. Work Environ. Health2(1), 1–13. 10.5271/sjweh.2827 (1976) - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
