

Ten-year outcomes after DMEK, DSAEK, and PK: insights on graft survival, endothelial cell density loss, rejection and visual acuity
- PMID: 39774993
- PMCID: PMC11707042
- DOI: 10.1038/s41598-025-85138-4
Ten-year outcomes after DMEK, DSAEK, and PK: insights on graft survival, endothelial cell density loss, rejection and visual acuity
Abstract
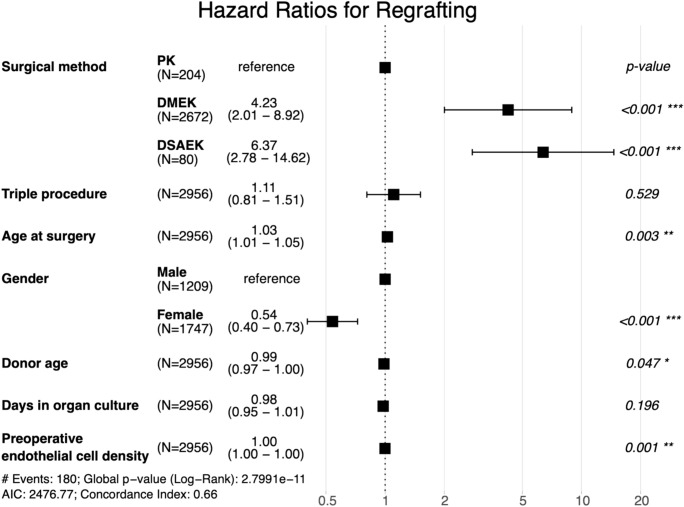
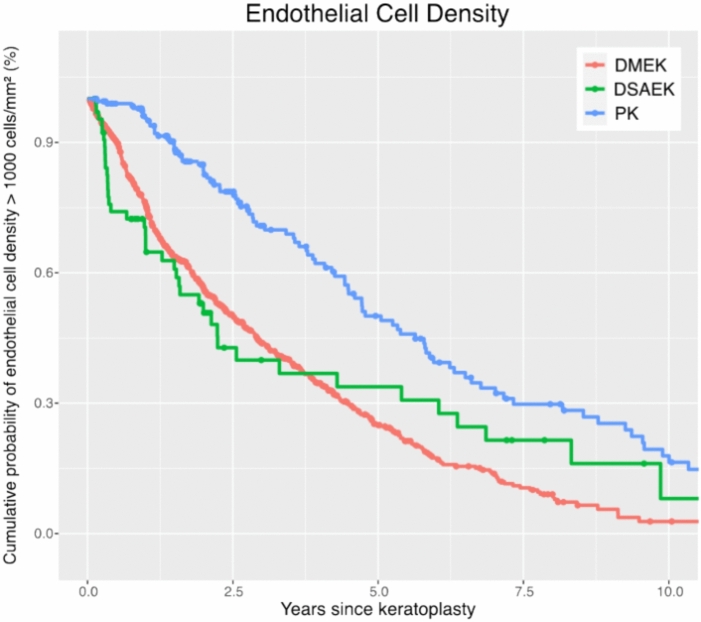
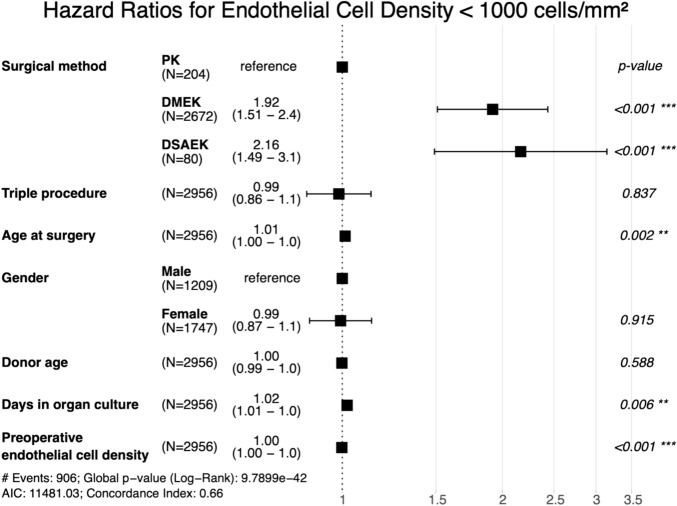
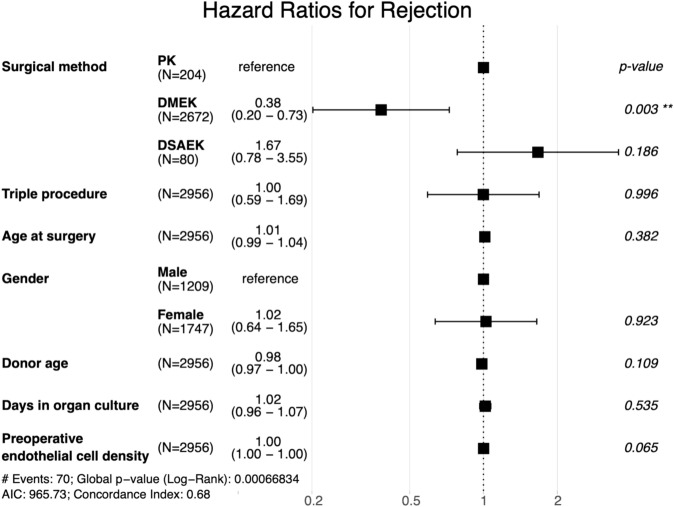
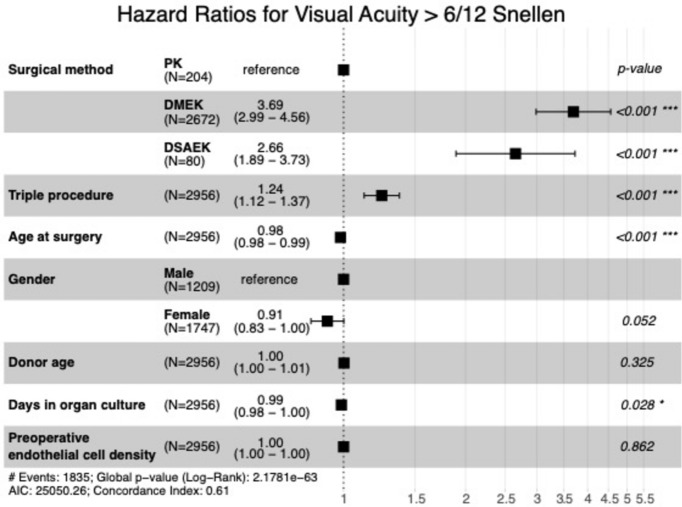
Fuchs Endothelial Corneal Dystrophy (FECD) is the most frequent indication for corneal transplantation, with Descemet membrane endothelial keratoplasty (DMEK), Descemet stripping automated endothelial keratoplasty (DSAEK), and penetrating keratoplasty (PK) being viable options. This retrospective study compared 10-year outcomes of these techniques in a large cohort of 2956 first-time keratoplasty eyes treated for FECD at a high-volume corneal transplant center in Germany. While DMEK and DSAEK provided faster visual recovery (median time to BSCVA ≥ 6/12 Snellen: DMEK 7.8 months, DSAEK 12.4 months, PK 37.9 months; cumulative probability of BSCVA ≥ 6/12 Snellen within 5 years: DMEK 93%, DSAEK 83%, PK 63%), PK surprisingly exhibited superior long-term graft survival (92% vs. 75% for DMEK and 73% for DSAEK at 10 years). Endothelial cell density (ECD) decreased significantly faster after DMEK and DSAEK, potentially contributing to their lower graft survival (10-year ECD > 1000 cells/mm2 probability: DMEK 3%, DSAEK 8%, PK 18%). DMEK demonstrated the lowest rejection rate (10% at 10 years vs. 13% for PK and 19% for DSAEK). These findings challenge the perceived superiority of endothelial keratoplasty and highlight the need for further investigation into the long-term implications of accelerated endothelial cell loss after DMEK and DSAEK.
Keywords: Corneal transplantation; DMEK; DSAEK; Fuchs endothelial corneal dystrophy; Graft survival; Penetrating keratoplasty.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Generative AI and AI-assisted technologies in the writing process: Grammarly v1.72.3.0, DeepL, GPT-4o, and Claude 3.5 Sonnet were used for linguistic improvements. The authors carefully checked the text suggestions for accuracy and made corrections where necessary. They take full responsibility for the publication’s content.
Figures




References
MeSH terms
LinkOut - more resources
Full Text Sources
