

Hospital and physician-based mental healthcare during 12 months of opioid agonist treatment for opioid use disorder: Exploring costs and factors associated with acute care
- PMID: 39775273
- PMCID: PMC11709258
- DOI: 10.1371/journal.pone.0314296
Hospital and physician-based mental healthcare during 12 months of opioid agonist treatment for opioid use disorder: Exploring costs and factors associated with acute care
Abstract
Background: Individuals with opioid use disorder (OUD) have a high prevalence of co-occurring mental health disorders; however, there exists little information on mental health service use for this population. We aimed to determine the prevalence of non-substance use-related mental health emergency department (ED) visits, hospitalizations, and outpatient physician visits for individuals receiving treatment for OUD over one year. We also explored individual-level characteristics associated with mental health care service use and estimated the costs of this care.
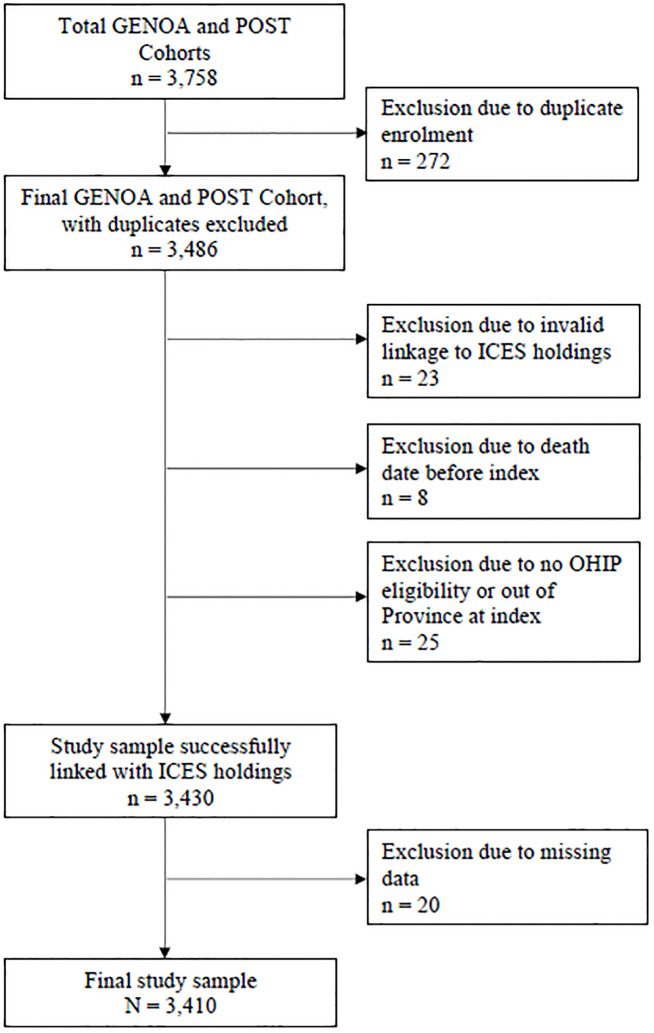
Methods: We linked observational cohort data collected from 3,430 individuals receiving treatment for OUD in Ontario, Canada, with health administrative records available for all individuals enrolled in Ontario's public health insurance program. Eligible participants were receiving medication treatment for OUD and were recruited between 2011 and 2021 Starting on the day of cohort enrolment, we included health service data for up to 12 months. We identified ED visits and hospitalizations for non-substance use-related mental health disorders using ICD-10-CA diagnostic codes. Outpatient mental health visits to primary care providers and psychiatrists were ascertained by examining the diagnostic codes of physician billing claims. We used logistic regression to explore the association between demographic and clinical factors of interest and mental health-related ED visits or hospitalizations. Mean one-year mental healthcare costs, calculated in 2022 Canadian dollars, were estimated. We fit a two-part zero-inflated negative binomial model to explore the association between factors of interest and healthcare costs.
Findings: Altogether, 14.9% of individuals had mental health-related acute care ED visits or hospitalizations and 37.3% had outpatient mental health visits during the follow up period. For participants with at least one visit, we determined the mean number of ED visits (1.93, standard deviation [SD] = 2.15), hospitalizations (1.46, SD = 1.05), primary care visits (3.51, SD = 4.31), and psychiatry visits (4.04, SD = 4.73). Lower odds of ED use and hospitalization were associated with older age (46+ compared to less than 25 years: odds ratio [OR] 0.43, 95% confidence interval [CI]: 0.29, 0.63) and being employed (OR 0.48, 95% CI 0.37, 0.61). Higher odds of ED use and hospitalization was associated with positive opioid urine drug screens (50% positive urine drug screens compared to 0%: OR 1.45, 95% CI 1.05, 2.01), having more comorbid conditions (7+ health conditions compared to 0-2 health conditions: OR 3.76, 95% CI 2.60, 5.44), and receipt of outpatient mental healthcare (OR 2.38, 95% CI 1.95, 2.92) were associated with higher odds of ED visits or hospitalizations. Mean one-year mental healthcare costs for individuals receiving ED visits or hospitalizations totaled $9,117.80 (95% CI 7,372.90, 10,862.70) per person. Mean one-year costs for individuals with outpatient mental healthcare alone totaled $382.30 (95% CI 343.20, 421.30) per person.
Conclusions: Individuals receiving treatment for OUD receive care in EDs, inpatient units, and outpatient clinics for mental health conditions other than substance use-related diagnoses. Healthcare costs were considerably higher for those receiving acute care treatment for mental health conditions. Studying integrated mental health and substance use disorder treatment in the outpatient setting should be a priority to bolster care for this population.
Copyright: © 2025 Rosic et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
References
-
- Gomes T, Murray R, Kolla G, Leece P, Kitchen S, Campbell T, et al. on behalf of the Ontario Drug Policy Research Network, Office of the Chief Coroner for Ontario and Ontario Agency for Health Protection and Promotion (Public Health Ontario). Patterns of medication and healthcare use among people who died of an opioid-related toxicity during the COVID-19 pandemic in Ontario. Toronto, ON: Ontario Drug Policy Research Network; 2022.
-
- Ahmad FB, Cisewski JA, Rossen LM, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. 2023.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
