

Association between demographic, clinical characteristics and severe complications by SARS-CoV-2 infection in a community-based healthcare network in Chile
- PMID: 39775294
- PMCID: PMC11684639
- DOI: 10.1371/journal.pone.0314376
Association between demographic, clinical characteristics and severe complications by SARS-CoV-2 infection in a community-based healthcare network in Chile
Abstract
Background: Most of the evidence on risk factors for COVID-19 complications comes from North America or Europe with very little research from Latin-America. We aimed to evaluate the association between sociodemographic, clinical factors and the risk of COVID-19 complications among adults in Chile, the fifth Latin-American country with more COVID-19 reported cases since de beginning of the Pandemic.
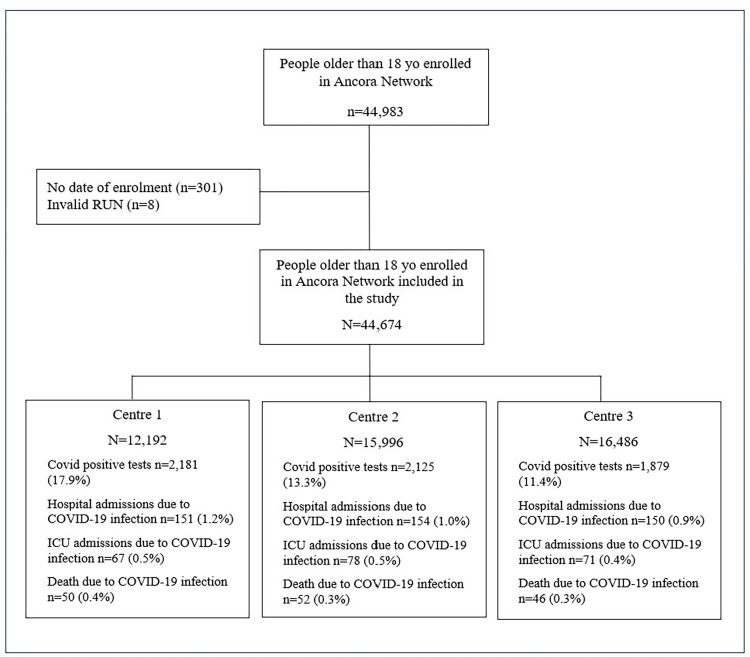
Methods: A retrospective population-based cohort study using data from electronic health records from a large Primary Care Network, linked to national hospital, immunization, Covid-19 PCR surveillance, mortality and birth records. We included people 18+ years old enrolled in the Primary Care Network between 1st January 2020 and 31st December 2021. Using Multivariate Cox proportional hazard models, we evaluate the association between sociodemographic, clinical characteristics with three COVID-19 complications: (1) a hospital admission, (2) an ICU admission, and (3) death due to a COVID-19 infection that occurred between the 1st January 2020 and the 31st December 2021.
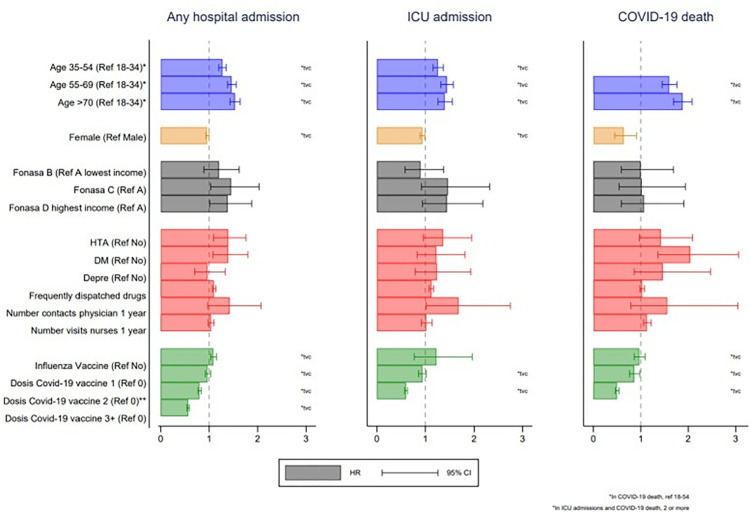
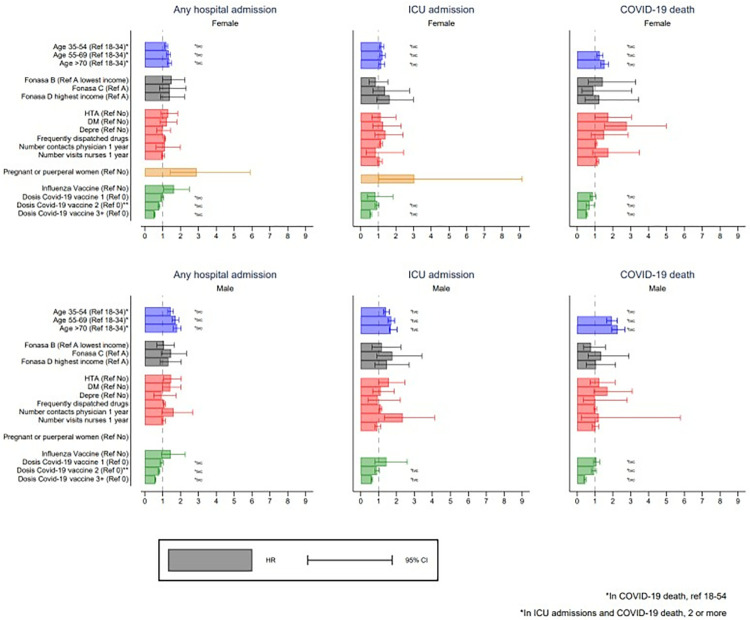
Results: 44,674 people were included. The mean age was 44.30 (sd 17.31), 55.6% were female, 15.9% had a type of healthcare insurance for people from the lowest category of income, 11.6% and 9.4% had a record of hypertension or diabetes mellitus diagnosis. Among the 44,674 people, 455 (1.02%) had a hospital admission due to a COVID-19 infection and 216(0.48%) of them also had an ICU admission. Among the 44,674 people,148(0.33%) died due to COVID-19 infection. Older age and male sex were consistently associated with a higher risk of the three COVID-19 complications. Hypertension and diabetes were associated with a higher risk of a hospital admission and death, but not with an ICU admissions due to COVID-19 infection. Having two or more COVID-19 vaccine doses compared with no doses was associated with a lower risk of any hospital admission (HR 0.81; 95% CI 0.77-0.84), an ICU admission (HR 0.60; 95% CI 0.57-0.63) and death (HR 0.50; 95% CI 0.46-0.54). Pregnant or puerperal women were more likely to be admitted to hospital (HR 2.89; 95% CI 1.41-5.89) or ICU (HR 3.04; 95% CI 1.01-9.14).
Conclusions: Sociodemographic and clinical factors associated with COVID-19 complications such as age, sex and pre-existing conditions were comparable to those reported in similar studies from higher-income countries, and can be used to predict severity in COVID-19 patients.
Copyright: © 2024 Leniz et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
