

Cerebral compliance assessment from intracranial pressure waveform analysis: Is a positional shift-related increase in intracranial pressure predictable?
- PMID: 39775319
- PMCID: PMC11684684
- DOI: 10.1371/journal.pone.0316167
Cerebral compliance assessment from intracranial pressure waveform analysis: Is a positional shift-related increase in intracranial pressure predictable?
Abstract
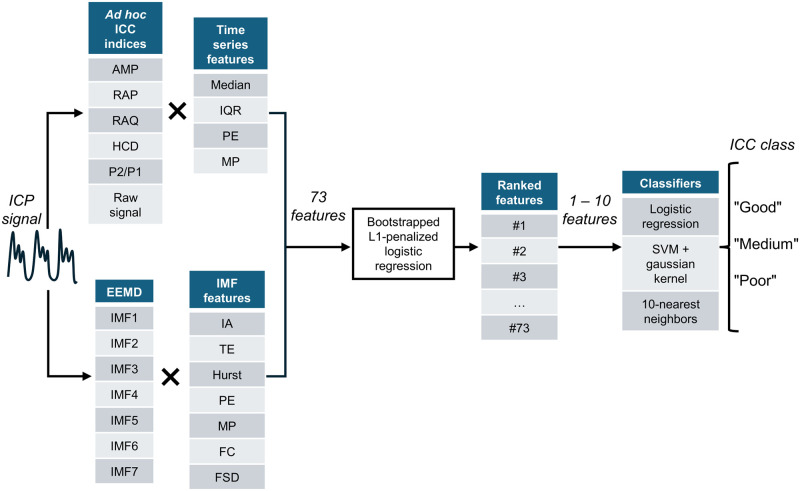
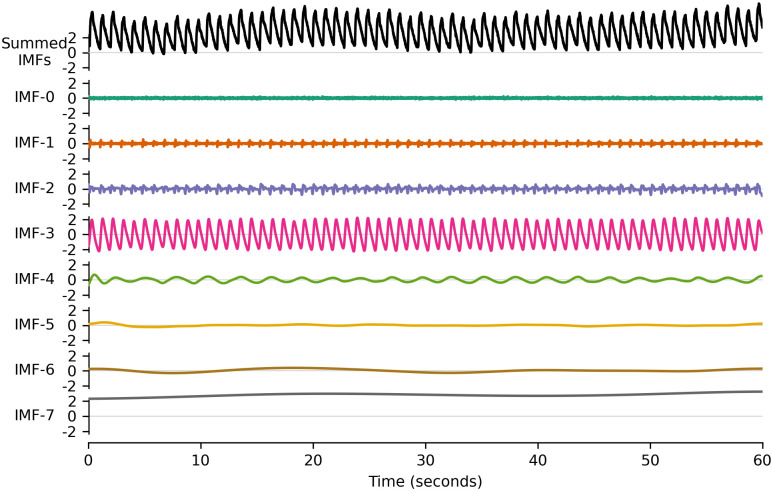
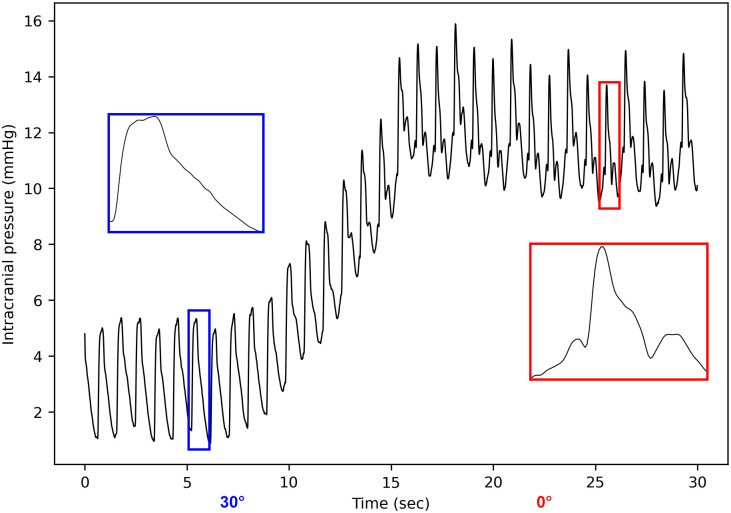
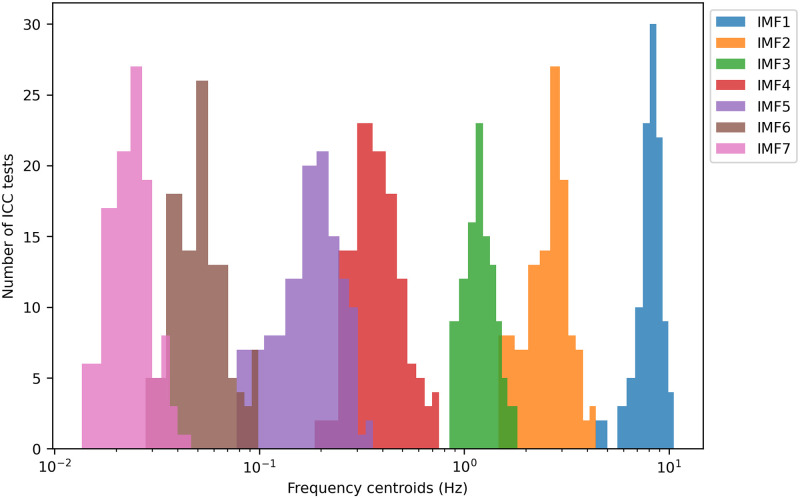
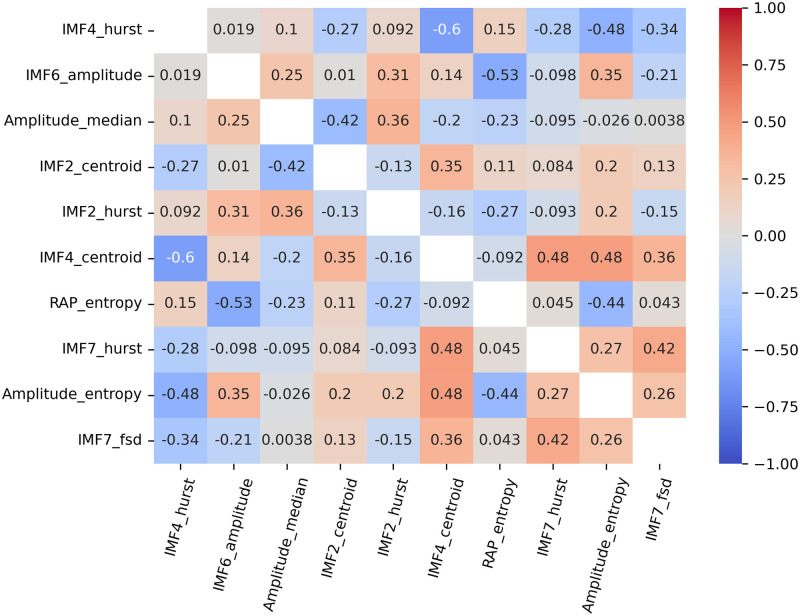
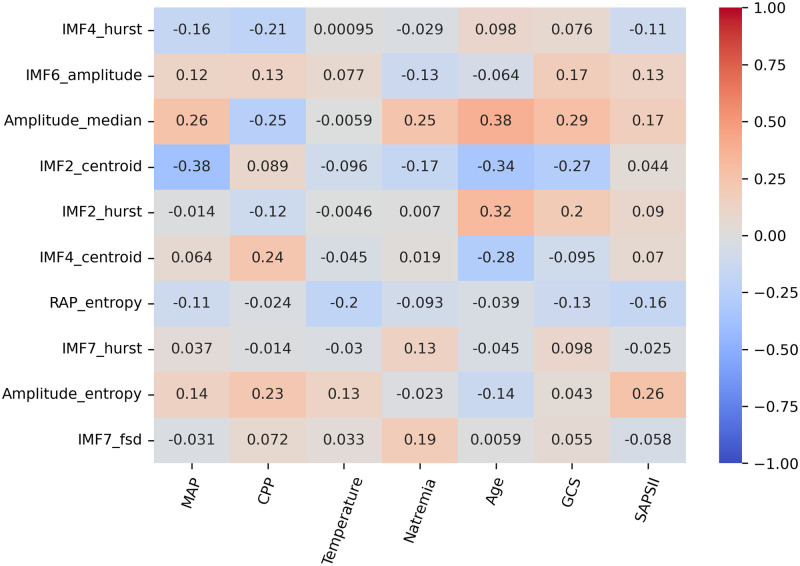
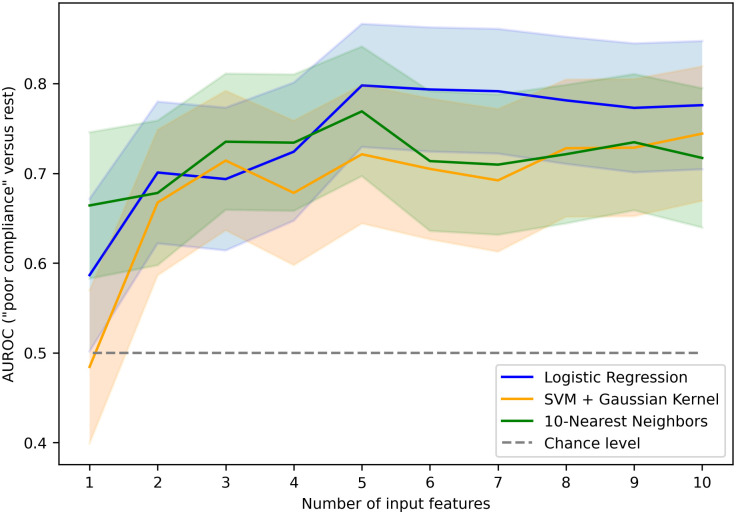
Real-time monitoring of intracranial pressure (ICP) is a routine part of neurocritical care in the management of brain injury. While mainly used to detect episodes of intracranial hypertension, the ICP signal is also indicative of the volume-pressure relationship within the cerebrospinal system, often referred to as intracranial compliance (ICC). Several ICP signal descriptors have been proposed in the literature as surrogates of ICC, but the possibilities of combining these are still unexplored. In the present study, a rapid ICC assessment consisting of a 30-degree postural shift was performed on a cohort of 54 brain-injured patients. 73 ICP signal features were calculated over the 20 minutes prior to the ICC test. After a selection step, different combinations of these features were provided as inputs to classification models. The goal was to predict the level of induced ICP elevation, which was categorized into three classes: less than 7 mmHg ("good ICC"), between 7 and 10 mmHg ("medium ICC"), and more than 10 mmHg ("poor ICC"). A logistic regression model fed with a combination of 5 ICP signal features discriminated the "poor ICC" class with an area under the receiving operator curve (AUROC) of 0.80 (95%-CI: [0.73-0.87]). The overall one-versus-one classification task was achieved with an averaged AUROC of 0.72 (95%-CI: [0.61-0.83]). Adding more features to the input set and/or using nonlinear machine learning algorithms did not significantly improve classification performance. This study highlights the potential value of analyzing the ICP signal independently to extract information about ICC status. At the patient's bedside, such univariate signal analysis could be implemented without dependence on a specific setup.
Copyright: © 2024 Legé et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
Marion Prud’homme and Donatien Legé are employees of Sophysa Company. Laurent Gergelé has performed consulting work for Sophysa Company. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Le Roux P, Menon DK, Citerio G, Vespa P, Bader MK, Brophy GM, et al. Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care: A statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Intensive Care Medicine. 2014;40(9):1189–1209. doi: 10.1007/s00134-014-3369-6 - DOI - PubMed
-
- Robba C, Graziano F, Rebora P, Elli F, Giussani C, Oddo M, et al. Intracranial pressure monitoring in patients with acute brain injury in the intensive care unit (SYNAPSE-ICU): an international, prospective observational cohort study. The Lancet Neurology. 2021;20(7):548–558. doi: 10.1016/S1474-4422(21)00138-1 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
