

The role of muscle synergies and task constraints on upper limb motor impairment after stroke
- PMID: 39775868
- PMCID: PMC11706858
- DOI: 10.1007/s00221-024-06953-1
The role of muscle synergies and task constraints on upper limb motor impairment after stroke
Abstract
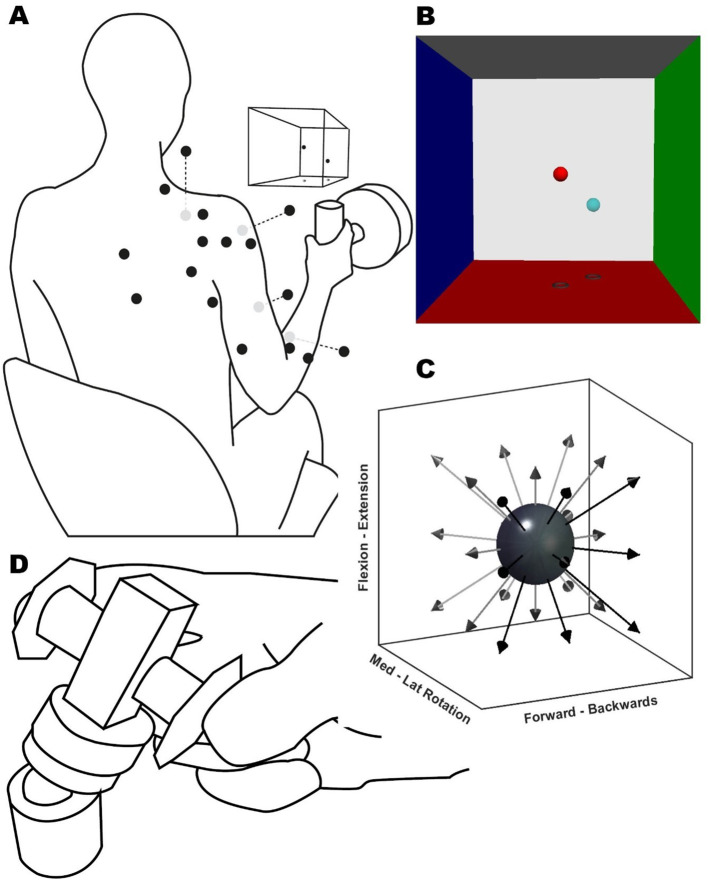
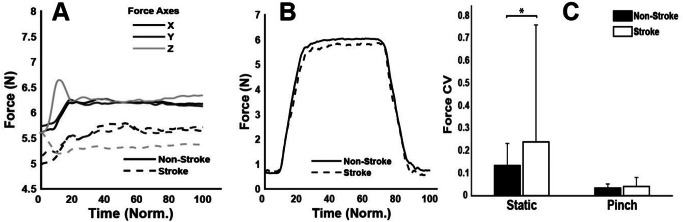
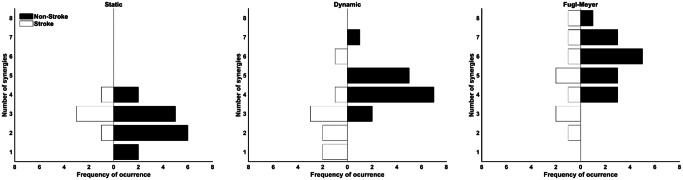
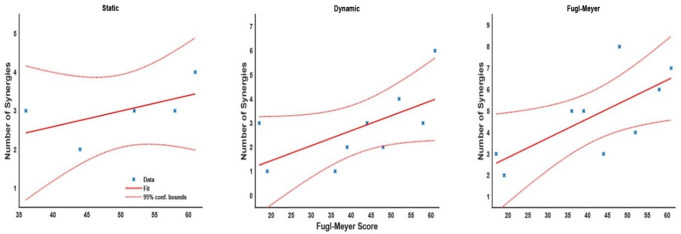
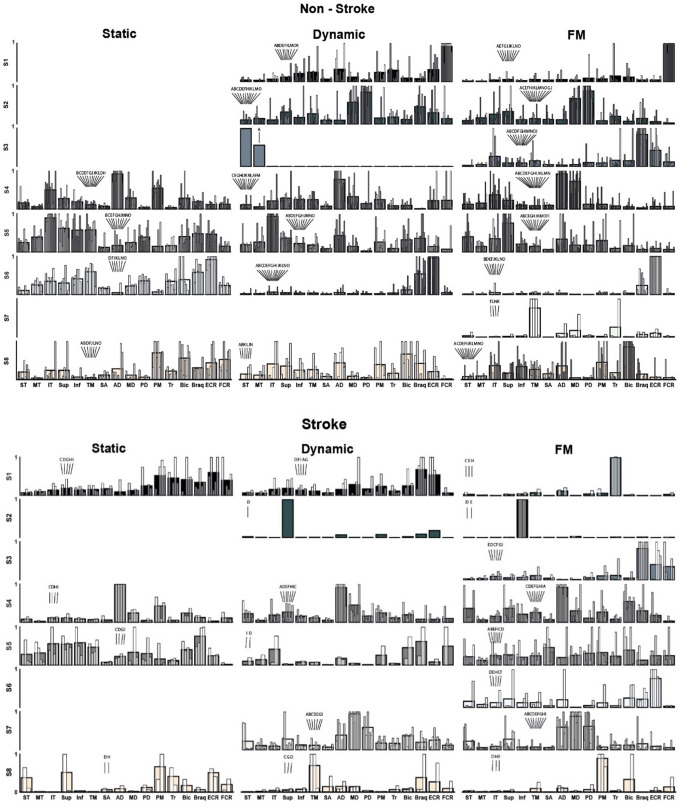
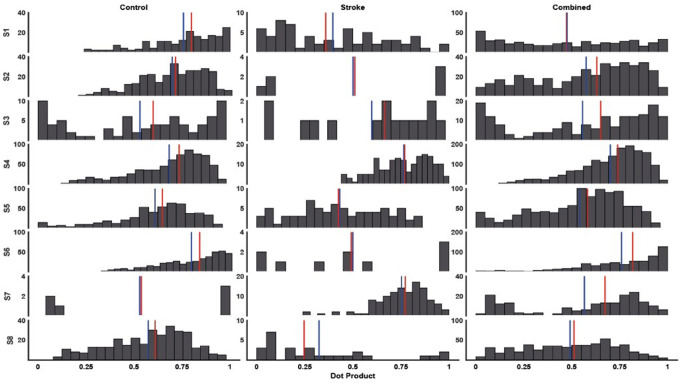
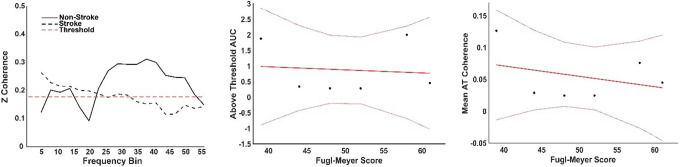
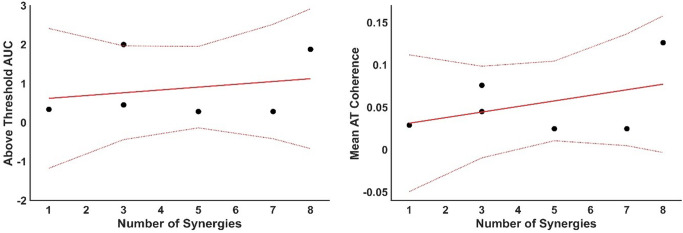
This study explores the role of task constraints over muscle synergies expression in the context of upper limb motor impairment after stroke. We recruited nine chronic stroke survivors with upper limb impairments and fifteen healthy controls, who performed a series of tasks designed to evoke muscle synergies through various spatial explorations. These tasks included an isometric force task, a dynamic reaching task, the clinical Fugl-Meyer (FM) assessment, and a pinch task. Electromyographic data from 16 upper limb muscles were collected during each task, alongside intermuscular coherence (IMC) measurements during the pinch task to assess neuromuscular connectivity. The findings confirm that motor impairment is inversely related to the diversity of muscle synergies, with fewer synergies and more stereotypical synergy structures observed post-stroke. The study further reveals that the nature of motor tasks significantly affects the number of identifiable muscle synergies, with less constrained tasks revealing a broader array of synergies. These findings highlight the importance of carefully selecting motor tasks in the context of clinical research and assessments to understand a patient's motor impairment, thus aiding in developing tailored rehabilitation strategies.
Keywords: FuglmMaeyer; Impairment; Motor control; Muscle synergies; Stroke; Upper limb.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The University of Auckland Human Participants Ethics Committee approved the research protocol and methods of the study (reference number 022246), and informed consent was gained before participation in any procedure. All experimental procedures and protocols were conducted by the Helsinki Declaration of 1975, revised in 2013, and approved by the institutional ethics committee. Consent for publication: All participants provided written informed consent, including consent for publication of anonymised data. Competing interests: The authors declare no conflicts of interest that could be perceived as potentially influencing the submitted work.
Figures
References
-
- Baker SN, Pinches EM, Lemon RN (2003) Synchronization in Monkey Motor Cortex during a Precision grip Task. II. Effect of Oscillatory Activity on Corticospinal output. J Neurophysiol 89(4):1941–1953. 10.1152/jn.00832.2002 - PubMed
-
- Barroso FO, Torricelli D, Molina-Rueda F, Alguacil-Diego IM, Cano-de-la-Cuerda R, Santos C, Moreno JC, Miangolarra-Page JC, Pons JL (2017) Combining muscle synergies and biomechanical analysis to assess gait in stroke patients. J Biomech 63:98–103. 10.1016/j.jbiomech.2017.08.006 - PubMed
-
- Berry MW, Browne M, Langville AN, Pauca VP, Plemmons RJ (2007) Algorithms and applications for approximate nonnegative matrix factorization. Comput Stat Data Anal 52(1):155–173. 10.1016/j.csda.2006.11.006
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
