

Biventricular dysfunction predicts mortality in ST elevation myocardial infarction patients with cardiogenic shock
- PMID: 39776021
- PMCID: PMC11711729
- DOI: 10.1186/s43044-024-00599-8
Biventricular dysfunction predicts mortality in ST elevation myocardial infarction patients with cardiogenic shock
Abstract
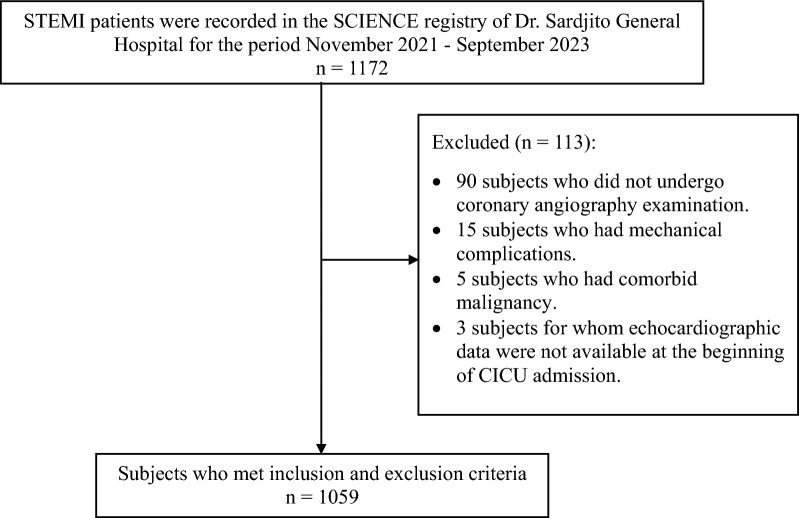
Background: The incidence of mortality in patients with cardiogenic shock due to ST elevation myocardial infarction (STEMI) remains high even with prompt reperfusion therapy. Ventricular systolic dysfunction is the primary condition causing cardiogenic shock in STEMI. Studies have been widely conducted on the left ventricle (LV) and right ventricle (RV) systolic dysfunction related to mortality events. However, the parameters of biventricular systolic dysfunction predicting mortality as a stronger predictor of mortality are still unclear. Accordingly, we evaluated the predictor mortality value of biventricular systolic dysfunction in STEMI patients with cardiogenic shocks. Based on The Society for Cardiovascular Angiography and Intervention classification, we analyzed data from November 2021 to September 2023 at Dr. Sardjito General Hospital in Yogyakarta, Indonesia, using the Sardjito Cardiovascular Intensive Care (SCIENCE) registry with a retrospective cohort design. Multivariate logistic regression analysis was used to assess predictors of in-hospital mortality.
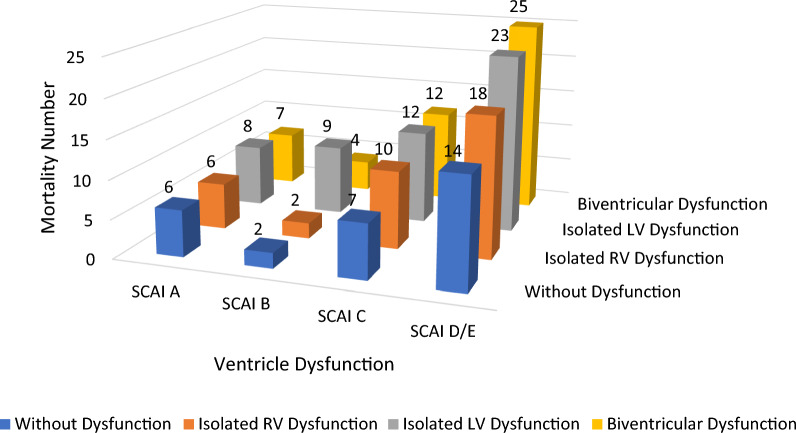
Results: There were 1,059 subjects with a mean ± SD age of 59 ± 11 years, dominated by men (80.5%) who met the inclusion and exclusion criteria. Based on multivariate analysis, biventricular dysfunction (BVD) is a factor that significantly increases the risk of in-hospital mortality (Odds ratio [OR], 1.771: 95% confidence interval [CI] 1.113-2.819; p = 0.016). Other significant factors affecting mortality were renal failure (OR, 5.122; 95% CI 3.233-8.116; p < 0.001), percutaneous coronary intervention (PCI) (OR, 0.493; 95% CI 0.248-0.981; p = 0.044), and inotropic/vasopressor (OR, 6.876; 95% CI 4.583-10.315; p < 0.001).
Conclusions: Biventricular dysfunction significantly increases the risk of in-hospital mortality in STEMI patients with cardiogenic shock. Renal failure, PCI, and the requirement for inotropic or vasopressor drugs are also factors that influence in-hospital mortality.
Keywords: Cardiogenic shock; Echocardiography; Mortality; ST elevated myocardial infarction.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study has been approved by the Medical and Health Research Ethics Committee of the Faculty of Medicine, Nursing and Public Health, Universitas Gadjah Mada, Yogyakarta, Indonesia, with number KE/FK/1707/EC/2023, and was conducted according to the ethical guidelines of the 2013 Declaration of Helsinki. The Institutional Medical Ethics Committee waived the requirement for informed consent for retrospectively enrolled patients. Consent for publication: Not applicable. Competing interests: The authors declare they have no competing interests.
Figures
Similar articles
-
Predictors of mortality in patients with cardiogenic shock treated with primary percutaneous coronary intervention and intra-aortic balloon counterpulsation.Med Klin Intensivmed Notfmed. 2016 Nov;111(8):715-722. doi: 10.1007/s00063-015-0118-8. Epub 2015 Nov 23. Med Klin Intensivmed Notfmed. 2016. PMID: 26596273 English.
-
Incidence and Predictors of Adverse Events Among Initially Stable ST-Elevation Myocardial Infarction Patients Following Primary Percutaneous Coronary Intervention.J Am Heart Assoc. 2022 Sep 6;11(17):e025572. doi: 10.1161/JAHA.122.025572. Epub 2022 Sep 3. J Am Heart Assoc. 2022. PMID: 36056738 Free PMC article.
-
Percutaneous Coronary Intervention in Older Patients With ST-Segment Elevation Myocardial Infarction and Cardiogenic Shock.J Am Coll Cardiol. 2019 Apr 23;73(15):1890-1900. doi: 10.1016/j.jacc.2019.01.055. J Am Coll Cardiol. 2019. PMID: 30999991 Free PMC article.
-
Culprit Vessel-Only Versus Multivessel Percutaneous Coronary Intervention in Patients With Cardiogenic Shock Complicating ST-Segment-Elevation Myocardial Infarction: A Collaborative Meta-Analysis.Circ Cardiovasc Interv. 2017 Nov;10(11):e005582. doi: 10.1161/CIRCINTERVENTIONS.117.005582. Circ Cardiovasc Interv. 2017. PMID: 29146672 Review.
-
Does multivessel revascularization fit all patients with STEMI and multivessel coronary artery disease? A systematic review and meta-analysis.Int J Cardiol Heart Vasc. 2021 Jun 11;35:100813. doi: 10.1016/j.ijcha.2021.100813. eCollection 2021 Aug. Int J Cardiol Heart Vasc. 2021. PMID: 34169144 Free PMC article. Review.
References
-
- Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS, Investigators N (2005) Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA 294(4):448–454. 10.1001/jama.294.4.448 - PubMed
-
- Helgestad OK, Josiassen J, Hassager C, Jensen LO, Holmvang L, Sørensen A et al (2019) Temporal trends in incidence and patient characteristics in cardiogenic shock following acute myocardial infarction from 2010 to 2017: a Danish cohort study. Eur J Heart Fail 21(11):1370–1378. 10.1002/ejhf.1566 - PubMed
-
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J (2009) Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction. Circulation 119(9):1211–1219. 10.1161/CIRCULATIONAHA.108.814947 - PMC - PubMed
-
- Pepe M, Santo Bortone A, Giordano A, Cecere A, Burattini O, Nestola PL et al (2020) Cardiogenic shock following acute myocardial infarction: What’s New? Shock 53(4):391–9 - PubMed
-
- Jacobs AK, Leopold JA, Bates E, Mendes LA, Sleeper LA, White H et al (2003) Cardiogenic shock caused by right ventricular infarction: a report from the SHOCK registry. J Am Coll Cardiol 41(8):1273–1279. 10.1016/s0735-1097(03)00120-7 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous