

Prophylactic direct oral anticoagulants vs. low molecular weight heparin after urological surgery: A systematic review and meta-analysis
- PMID: 39776556
- PMCID: PMC11702991
- DOI: 10.1080/20905998.2024.2395202
Prophylactic direct oral anticoagulants vs. low molecular weight heparin after urological surgery: A systematic review and meta-analysis
Abstract
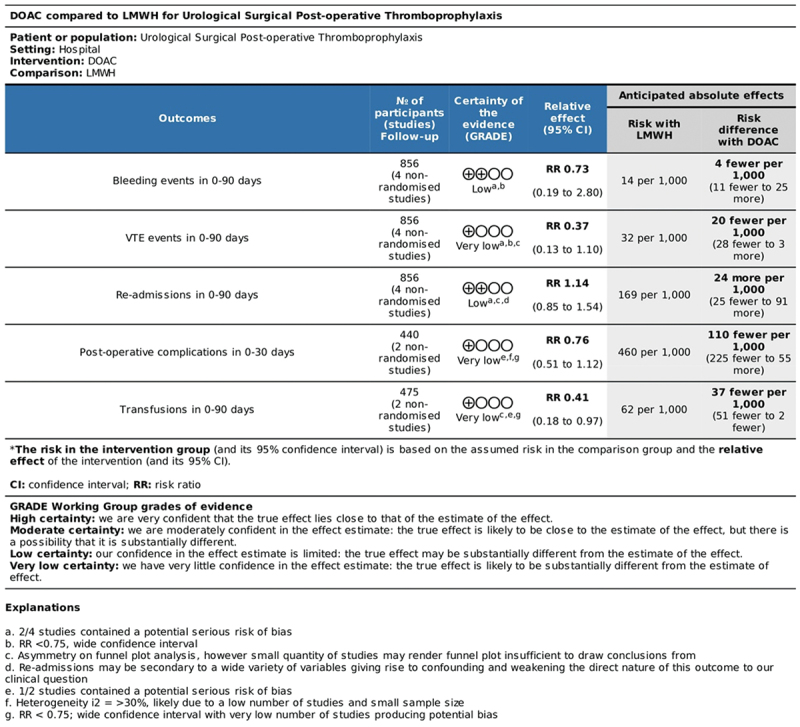
Purpose: To compare the outcomes of using prophylactic direct oral anti-coagulants (DOAC) and low-molecular-weight heparin (LMWH) after major urologic surgery.
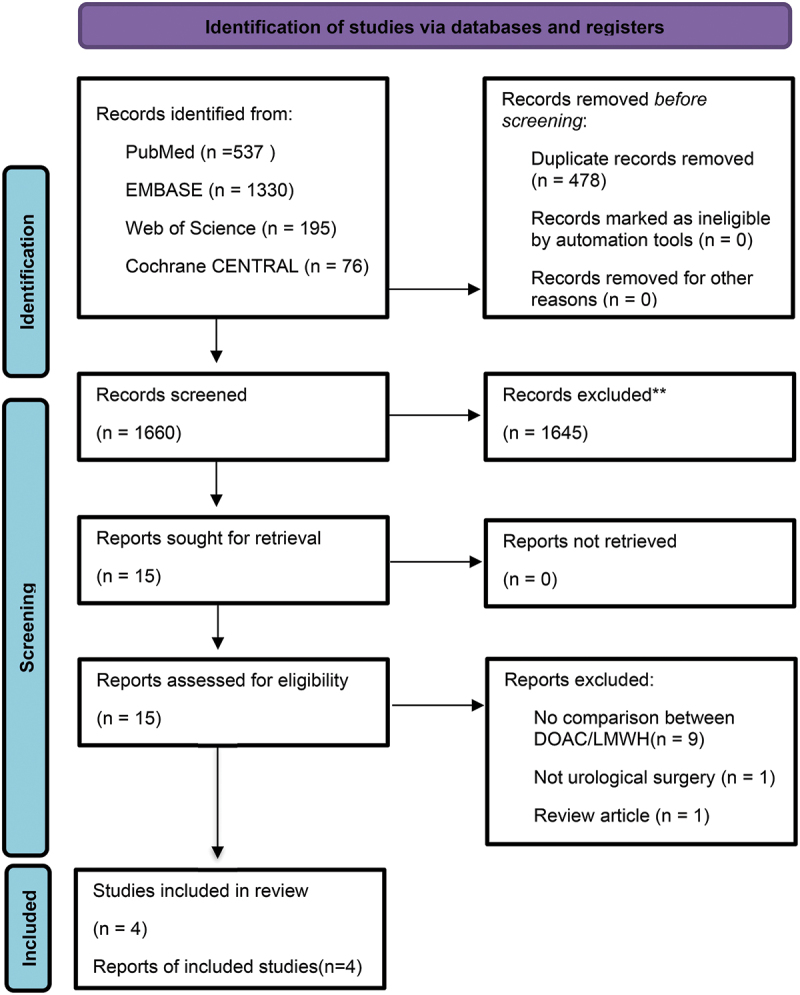
Materials and methods: Systematic literature searches of MEDLINE, Embase, Web of Science, and Cochrane CENTRAL were performed up to 9 November 2023, and protocols were registered on PROSPERO (CRD42024494424). The primary outcomes were post-operative incidence of VTE and bleeding. The secondary outcomes included re-admissions and transfusions needed, post-operative complications and exploring the radical cystectomy sub-group. Outcomes were reported in 30 and 90 days where feasible with sub-group analysis.
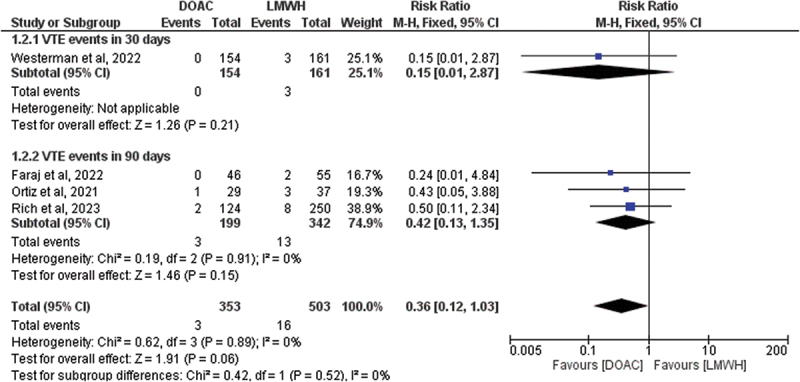
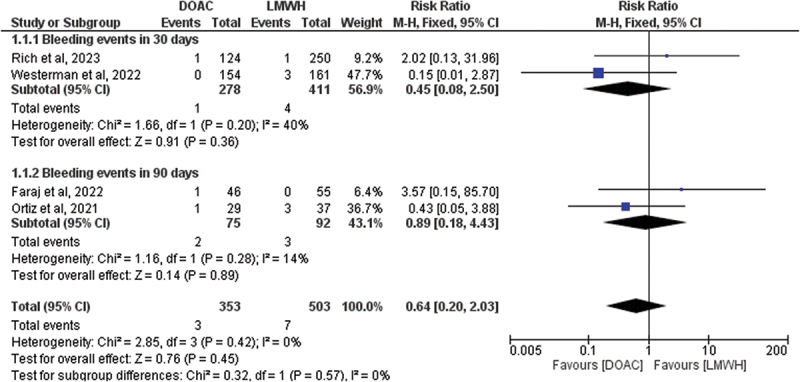
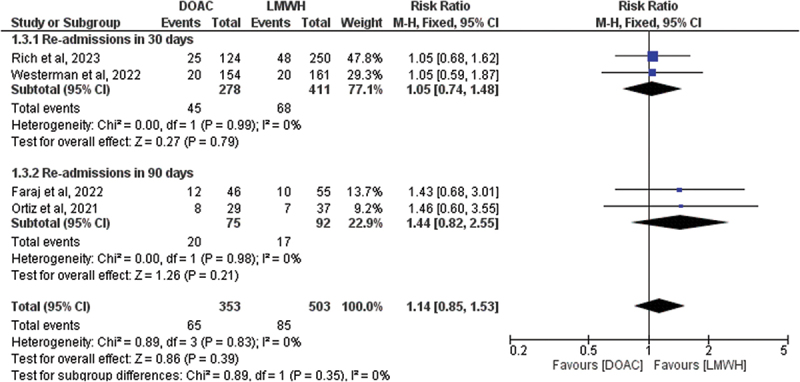
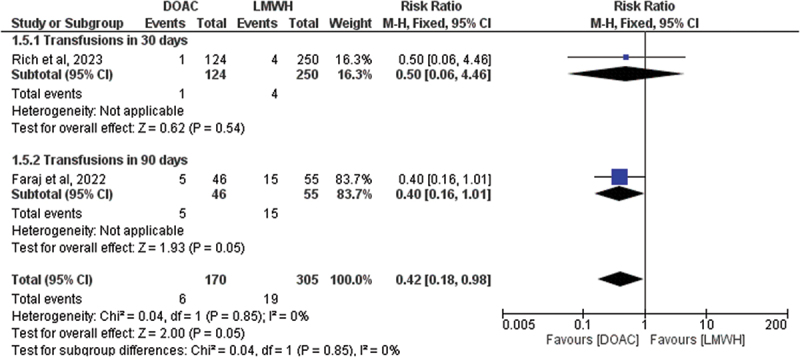
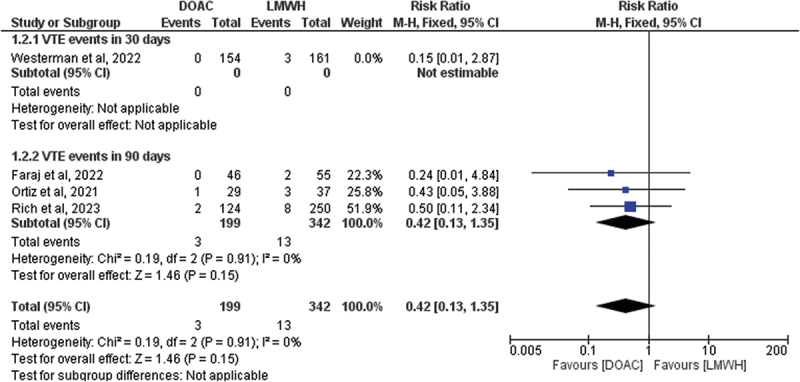
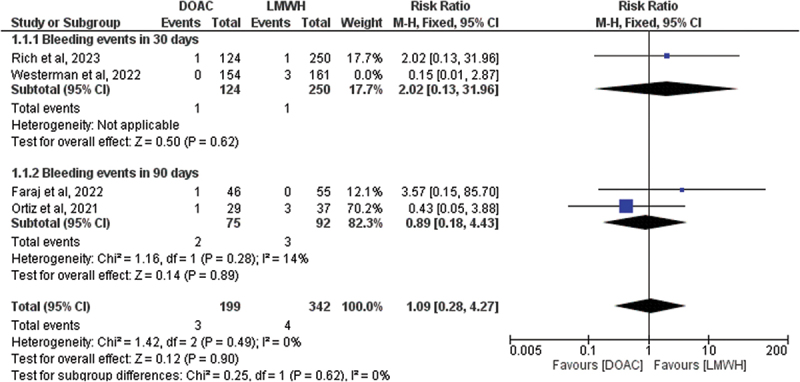
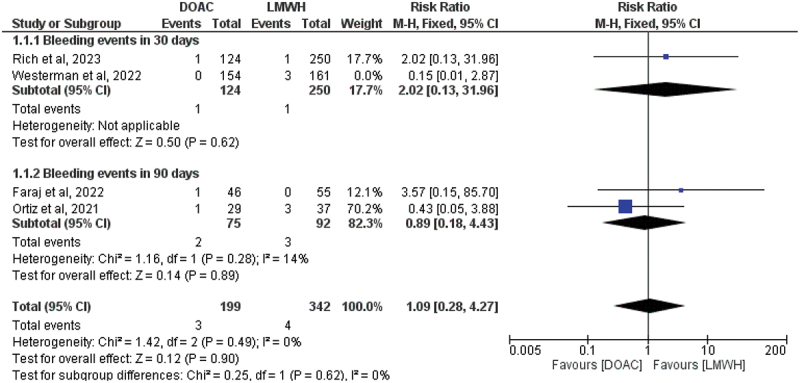
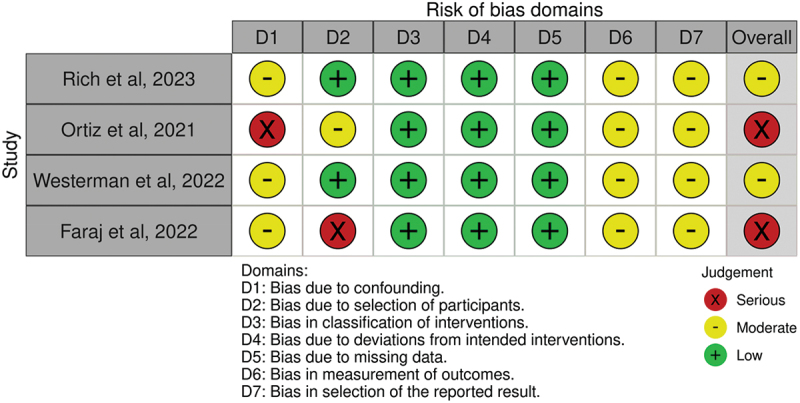
Results: Searches yielded four studies that included 856 patients and the outcomes were reported within 30 and 90 days, with sub-analysis performed for each time-interval. We found no statistically significant differences between DOAC and LWMH within neither primary nor secondary outcomes; VTE events (RR 0.36; p = 0.06); bleeding events (RR 0.64; p = 0.45); re-admissions (RR 1.14; p = 0.39); transfusions (RR 0.42; p = 0.05) within 0-90 days and post-operative complications within 30 days (RR 0.76; p = 0.17). Similar results were found when exploring radical cystectomy sub-group: VTE risk (RR 0.42, p = 0.15), bleeding risk (RR 1.09; p = 0.90), and re-admissions to hospital (RR 1.18, p = 0.35). Limitations include small sample size, and difficult generalization to all urological surgery as most of the analyzed cohort underwent radical cystectomy.
Conclusion: DOACs may be a safe and possibly cost-effective alternative to LMWH as post-operative thromboprophylaxis. However, these findings should be interpreted with caution due to limitations; therefore, more randomized studies are needed to ascertain our findings.
Keywords: Urology; direct oral anticoagulant; low-molecular-weight heparin; radical cystectomy; surgery; venous thromboembolism.
© 2024 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources