

C-X-C motif chemokine receptor 4-directed PET signal in the arterial tree is not consistently linked to calcified plaque burden and cardiovascular risk
- PMID: 39776816
- PMCID: PMC11700869
- DOI: 10.7150/thno.102910
C-X-C motif chemokine receptor 4-directed PET signal in the arterial tree is not consistently linked to calcified plaque burden and cardiovascular risk
Abstract
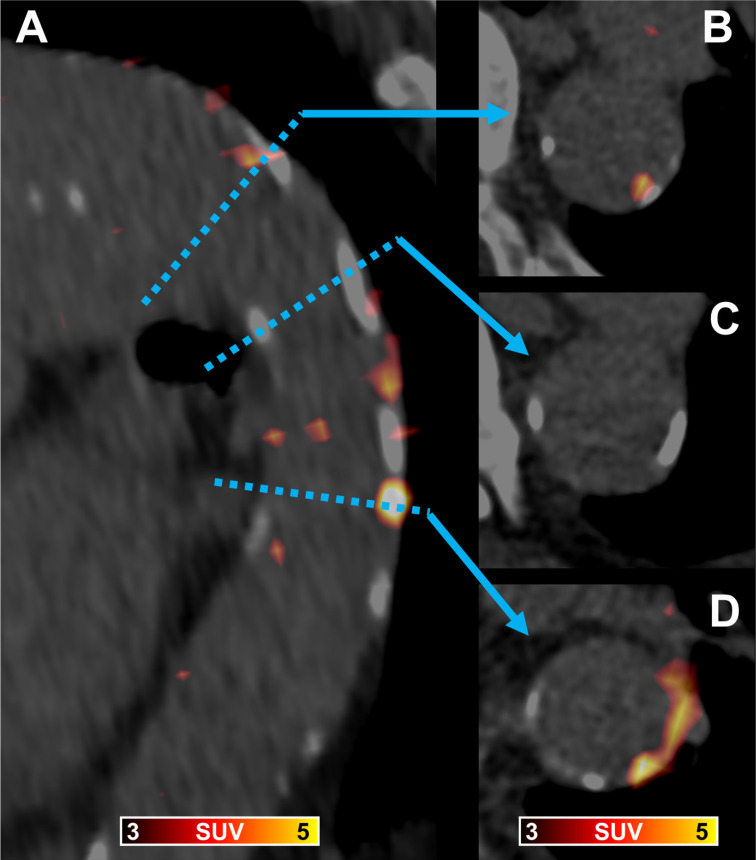
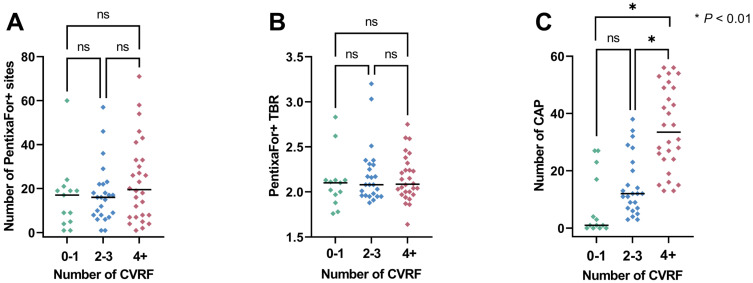
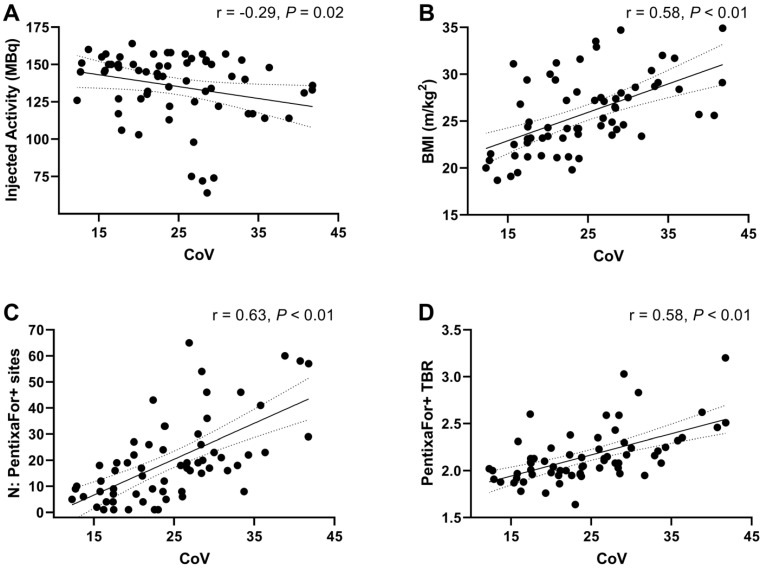
Purpose: To establish the extent, distribution and frequency of in-vivo vessel wall [68Ga]Ga-PentixaFor uptake and to determine its relationship with calcified atherosclerotic plaque burden (CAP) and cardiovascular risk factors (CVRF). Methods: 65 oncological patients undergoing [68Ga]Ga-PentixaFor PET/CT were assessed. Radiotracer uptake (target-to-background ratio [TBR]) and CAP burden (including number of CAP sites, calcification circumference and thickness) in seven major vessel segments per patient were determined. We then investigated associations of vessel wall uptake with CAP burden, cardiovascular risk (CVRF and European Society of Cardiology [ESC] SCORE2/SCORE2-OP risk chart) and image noise (determined by coefficient of variation [CoV] from unaffected liver parenchyma). Results: We identified 1292 sites of high focal [68Ga]Ga-PentixaFor uptake (PentixaFor+ sites) in the vessel wall in 65/65 (100%) patients, with concomitant calcification in 385/1292 (29.8%) sites. There were no significant associations between vessel wall uptake and CAP burden (number of PentixaFor+ sites: r ≤ 0.18, P ≥ 0.14; PentixaFor+ TBR: r ≤ 0.08, P ≥ 0.54). The number of PentixaFor+ sites showed a moderate correlation with cardiovascular risk (ESC SCORE2/SCORE2-OP, r = 0.30; number of CVRF, r = 0.26; P = 0.04, respectively), but failed to reach significance for PentixaFor+ TBR (r ≤ 0.18, P ≥ 0.22). In univariable regression analysis, body mass index (odds ratio [OR] 1.08, 95%-confidence interval [CI] 1.02-1.14) and CoV (OR, 1.07; CI, 1.05-1.10) were linked to TBR and the number of PentixaFor+ sites (P < 0.01, respectively), while injected activity was only associated with the latter imaging parameter (OR, 0.99; CI, 0.98-1.00; P = 0.04). In multivariable regression, injected activity (OR, 1.00; CI, 0.99-1.00) and CoV (OR, 1.06; CI, 1.06-1.07) remained significantly associated with the number of PentixaFor+ sites (P < 0.01, respectively). CoV, however, was the only parameter significantly linked to PentixaFor+ TBR on multivariable analysis (OR, 1.02; CI, 1.01-1.03; P < 0.01). Conclusion: On a visual and quantitative level, high focal [68Ga]Ga-PentixaFor uptake in the arterial tree was not consistently linked to vessel wall calcification or cardiovascular risk. Image noise, however, may account for a substantial portion of apparent vessel wall uptake.
Keywords: C-X-C motif chemokine receptor 4; CXCR4; [68Ga]Ga-PentixaFor; atherosclerosis; cardiovascular risk factors; molecular imaging.
© The author(s).
Conflict of interest statement
Competing Interests: RAW and AKB have received speaker honoraria from Novartis/AAA and PentixaPharm. RAW reports advisory board work for Novartis/AAA and Bayer. AKB is a member of the advisory board of PentixaPharm. All other authors declare no conflict of interest.
Figures

Similar articles
-
Molecular imaging of arterial fibroblast activation protein: association with calcified plaque burden and cardiovascular risk factors.Eur J Nucl Med Mol Imaging. 2023 Aug;50(10):3011-3021. doi: 10.1007/s00259-023-06245-w. Epub 2023 May 6. Eur J Nucl Med Mol Imaging. 2023. PMID: 37147478 Free PMC article.
-
Clinical Molecular Imaging of Chemokine Receptor CXCR4 Expression in Atherosclerotic Plaque Using 68Ga-Pentixafor PET: Correlation with Cardiovascular Risk Factors and Calcified Plaque Burden.J Nucl Med. 2018 Feb;59(2):266-272. doi: 10.2967/jnumed.117.196485. Epub 2017 Aug 3. J Nucl Med. 2018. PMID: 28775206
-
[68Ga]Pentixafor-PET/MRI for the detection of Chemokine receptor 4 expression in atherosclerotic plaques.Eur J Nucl Med Mol Imaging. 2018 Apr;45(4):558-566. doi: 10.1007/s00259-017-3831-0. Epub 2017 Sep 21. Eur J Nucl Med Mol Imaging. 2018. PMID: 28932900 Free PMC article.
-
Imaging findings and clinical relevance of 68Ga-Pentixafor PET in atherosclerosis: a systematic review.BMC Med Imaging. 2023 Oct 26;23(1):166. doi: 10.1186/s12880-023-01134-y. BMC Med Imaging. 2023. PMID: 37884885 Free PMC article.
-
Advances in PET Imaging of the CXCR4 Receptor: [68Ga]Ga-PentixaFor.Semin Nucl Med. 2024 Jan;54(1):163-170. doi: 10.1053/j.semnuclmed.2023.09.002. Epub 2023 Nov 3. Semin Nucl Med. 2024. PMID: 37923671 Free PMC article. Review.
References
-
- Zlotnik A, Burkhardt AM, Homey B. Homeostatic chemokine receptors and organ-specific metastasis. Nat Rev Immunol. 2011;11:597–606. - PubMed
-
- Domanska UM, Kruizinga RC, Nagengast WB, Timmer-Bosscha H, Huls G, de Vries EG. et al. A review on CXCR4/CXCL12 axis in oncology: no place to hide. Eur J Cancer. 2013;49:219–30. - PubMed
-
- Guo F, Wang Y, Liu J, Mok SC, Xue F, Zhang W. CXCL12/CXCR4: a symbiotic bridge linking cancer cells and their stromal neighbors in oncogenic communication networks. Oncogene. 2016;35:816–26. - PubMed
-
- Scala S. Molecular Pathways: Targeting the CXCR4-CXCL12 Axis-Untapped Potential in the Tumor Microenvironment. Clin Cancer Res. 2015;21:4278–85. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
