

Self-Administered Traction as an Adjunct in the Chiropractic Treatment of Low Back Pain: A Case Report
- PMID: 39776823
- PMCID: PMC11701848
- DOI: 10.1016/j.jcm.2024.08.005
Self-Administered Traction as an Adjunct in the Chiropractic Treatment of Low Back Pain: A Case Report
Abstract
Objective: The purpose of this case report is to describe self-administered lumbar traction as a component of the treatment of a patient with low back pain (LBP).
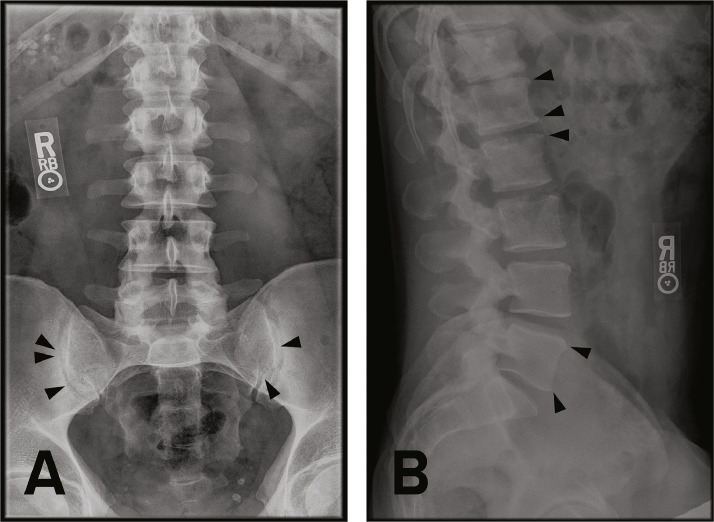
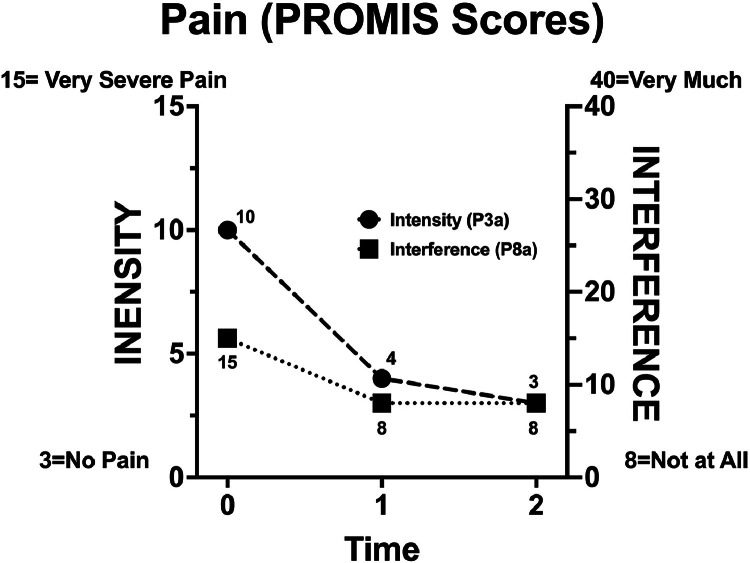
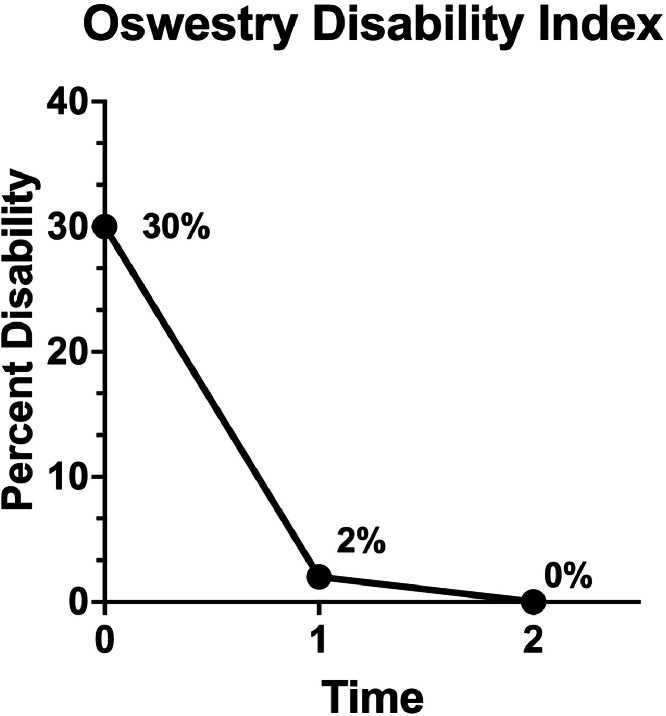
Clinical features: A 41-year-old male chiropractic student presented with an exacerbation of intermittent LBP of approximately 2 years duration. Pain intensity was 4 to 8/10 on a verbal pain scale the day after exertion and 10 on the Patient Reported Outcomes Measurement Information System (PROMIS) 3a. Pain interference was 15 on the PROMIS-8a. The Oswestry Disability Index was 30%. Radiographs showed mild bilateral arthritic changes throughout the lumbar spine and sacroiliac joints. Diagnoses of acute exacerbation of recurrent, mechanical low back pain with thoracic and lumbar segmental dysfunction, lumbosacral spondylosis without myelopathy, and bilateral sacroiliac joint arthritis were made.
Intervention and outcomes: The student received 14 treatments over 5 weeks consisting of spinal manipulation and therapeutic exercises in conjunction with clinician-supervised, self-administered traction. After 14 treatments, the patient was discharged, reporting resolution of LBP (pain intensity [PROMIS-3a] = 4; pain interference [PROMIS-8a] = 8; Oswestry 2%; and increased range of motion). Pain resolution remained for more than 2 years without additional treatment (pain intensity = 3; pain interference = 8; Oswestry 0%; continued increased range of motion).
Conclusion: The patient reported long-term benefit from a course of spinal manipulation and therapeutic exercises in conjunction with novel self-administered traction with flexion.
Keywords: Case report; Chiropractic; Low back pain; Spine; Traction.
© 2024 by National University of Health Sciences.
Figures

References
-
- Buchbinder R, Batterham R, Elsworth G, Dionne CE, Irvin E, Osborne RH. A validity-driven approach to the understanding of the personal and societal burden of low back pain: development of a conceptual and measurement model. Arthritis Res Ther. 2011;13(5):R152. doi: 10.1186/ar3468. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
