

A comparative analysis of unilateral biportal endoscopic and open laminectomy in multilevel lumbar stenosis
- PMID: 39777310
- PMCID: PMC11704811
- DOI: 10.3389/fneur.2024.1409088
A comparative analysis of unilateral biportal endoscopic and open laminectomy in multilevel lumbar stenosis
Abstract
Background: Approximately 103 million people across the globe suffer from symptomatic lumbar spinal stenosis, impacting their health and quality of life. The unilateral biportal endoscopic technique is effective for treating single-segment degenerative lumbar spinal stenosis and is seen as a viable alternative to traditional open lumbar laminectomy. However, research on the application of this technique for multilevel lumbar spinal stenosis remains lacking.
Objective: To compare the clinical effects of unilateral biportal endoscopy (UBE) and open lumbar decompression (OLD) in the treatment of multilevel lumbar spinal stenosis (MLSS).
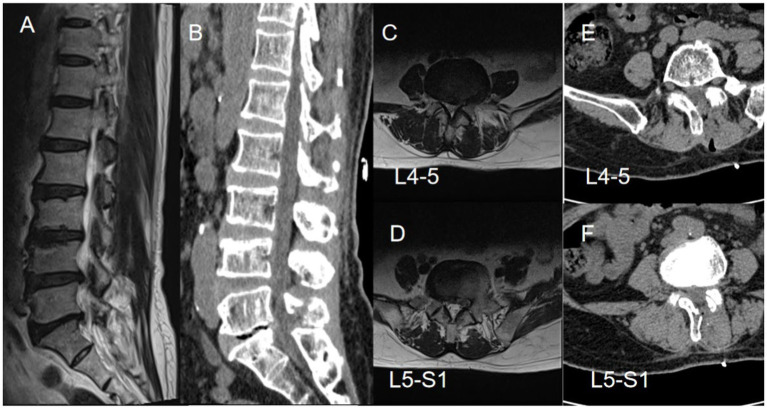
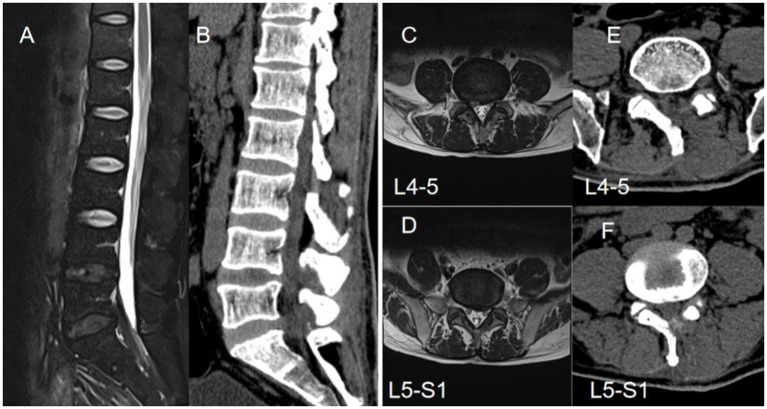
Methods: This retrospective study was conducted from February 2019 to December 2023 and compared the outcomes of Multilevel UBE surgery to OLD. The included patients were divided into two groups, namely the UBE group (n = 42, 86 surgical segments) and the OLD group (n = 40, 82 surgical segments). At the 1-year follow-up, the imaging findings, visual analogue scale (VAS), Oswestry disability index (ODI), and Zurich Claudication Questionnaire (ZCQ) were assessed. MRI measurements of the dural sac (CSA) and paravertebral cross-sectional area (PMA) were taken before surgery and at the final follow-up.
Results: The surgical segments of the two groups primarily consisted of adjacent segments (UBE 78.6% vs. OLD 78.8%), with a higher proportion of bilateral decompression in the OLD group (UBE 24.4% vs. OLD 28.0%). Preoperative imaging evaluation indicated a higher prevalence of grade C (severe stenosis) compared to grade D (severe stenosis) in both groups (UBE 74.4% vs. OLD 72%). The OLD group exhibited significantly greater blood loss compared to the UBE group (147.63 ± 26.55 vs. 46.19 ± 25.25 mL, p < 0.001). In addition, the duration of hospitalization in the OLD group was notably longer compared to the UBE group (7.58 ± 1.39 vs. 4.38 ± 1.56 days, p < 0.05). Paravertebral muscle atrophy (PMA) in the UBE group was significantly lower than in the OLD group (3.49 ± 3.03 vs. 5.58 ± 3.00, p < 0.05). Significantly elevated serum creatine kinase (CK) levels were observed in both groups, peaking at 1-day post-surgery, with the UBE group showing significantly lower levels than the OLD group (108.1 ± 12.2 vs. 364.13 ± 20.24 U/L, p < 0.05). On postoperative day 7, a significant decrease in liver enzyme levels was found in UBE group compared to the preoperative levels (61.81 ± 7.14 vs. 66.10 ± 8.26 U/L, p < 0.05). The Oswestry Disability Index (ODI) and Zurich Claudication Questionnaire (ZCQ) scores at 1 week, 6 months, and 1 year post-operation showed significant improvement compared to the preoperative scores in both groups (p < 0.05). The study found statistically significant differences in both the Visual Analog Scale (VAS) score (2.28 ± 0.59 vs. 2.85 ± 0.74, p < 0.05) and the Oswestry Disability Index (ODI) score (36.28 ± 2.03 vs. 37.57 ± 1.98, p < 0.05) at 1 week post-surgery between the two groups. However, no significant variations in scores were noted between preoperative and postoperative time points at other follow-up intervals.
Conclusion: The unilateral biportal endoscopic technique was applied to treat multilevel lumbar spinal stenosis, demonstrating decreased intraoperative bleeding and lower postoperative muscle-related complications compared to open lumbar decompression. Furthermore, UBE was found to promote early mobilization.
Keywords: multilevel lumbar spinal stenosis; open lumbar decompression; spinal endoscopy; unilateral approach bilateral decompression; unilateral biportal endoscopy.
Copyright © 2024 Ouyang, Yang, Chen, Li, Zheng, Luo and Tan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Decompression via unilateral biportal endoscopy for severe degenerative lumbar spinal stenosis: A comparative study with decompression via open discectomy.Front Neurol. 2023 Feb 22;14:1132698. doi: 10.3389/fneur.2023.1132698. eCollection 2023. Front Neurol. 2023. PMID: 36908592 Free PMC article.
-
[Comparative study of decompression of unilateral biportal endoscopic compared to laminectomy with fusion and internal fixation in the treatment of severe lumbar spinal stenosis].Zhonghua Yi Xue Za Zhi. 2022 Nov 8;102(41):3281-3287. doi: 10.3760/cma.j.cn112137-20220720-01583. Zhonghua Yi Xue Za Zhi. 2022. PMID: 36319180 Chinese.
-
Comparison of Biportal Endoscopic Technique and Conventional Unilateral Laminectomy for Bilateral Decompression (ULBD) for Multi-Level Degenerative Lumbar Spinal Stenosis in Elderly People.Orthop Surg. 2025 Aug;17(8):2302-2312. doi: 10.1111/os.70084. Epub 2025 Jun 17. Orthop Surg. 2025. PMID: 40528425 Free PMC article.
-
Unilateral Endoscopic and Unilateral Biportal Endoscopic surgery for lumbar spinal stenosis: a systematic review and meta-analysis.Front Surg. 2025 Jun 16;12:1585783. doi: 10.3389/fsurg.2025.1585783. eCollection 2025. Front Surg. 2025. PMID: 40589530 Free PMC article.
-
Unilateral biportal endoscopic spine surgery for lumbar spinal stenosis: a systematic review and meta-analysis.Eur Rev Med Pharmacol Sci. 2023 Jun;27(11):4998-5012. doi: 10.26355/eurrev_202306_32617. Eur Rev Med Pharmacol Sci. 2023. PMID: 37318474
References
-
- Awaya T, Nishimura Y, Eguchi K, Nagashima Y, Ando R, Akahori S, et al. . Radiological analysis of minimally invasive microscopic laminectomy for Lumbar Canal stenosis with a focus on multilevel stenosis and spondylolisthesis. World Neurosurg. (2022) 164:e224. doi: 10.1016/j.wneu.2022.04.079, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials