

Selective otolithic dysfunction in patients presenting with acute spontaneous vertigo: consideration based on MRI
- PMID: 39777315
- PMCID: PMC11704425
- DOI: 10.3389/fneur.2024.1517112
Selective otolithic dysfunction in patients presenting with acute spontaneous vertigo: consideration based on MRI
Abstract
Objective: Acute unilateral peripheral vestibulopathy or vestibular neuritis (AUPV/VN) manifests as acute onset vertigo, often accompanied by nausea, vomiting, and moderate gait instability. It is suspected when vestibular hypofunction is documented on video-head impulse (video-HITs) and caloric tests in the presence of contralesionally beating horizontal-torsional nystagmus. Herein, we report patients presenting with acute vestibular syndrome (AVS) showing selective otolithic dysfunction in the presence of normal caloric and video-HITs and abnormal enhancement of the peripheral vestibular structures on MRI.
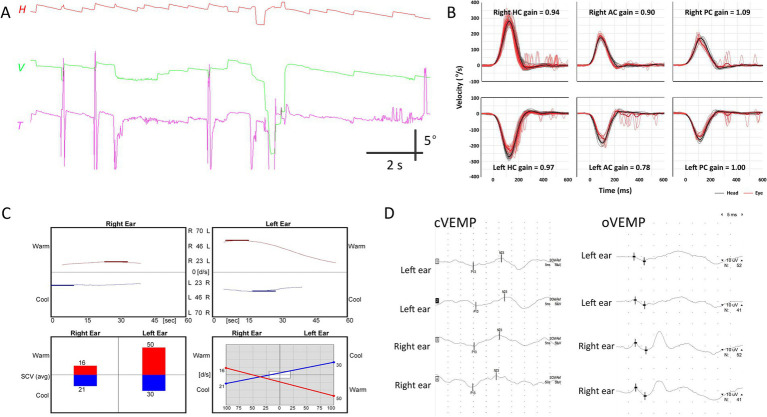
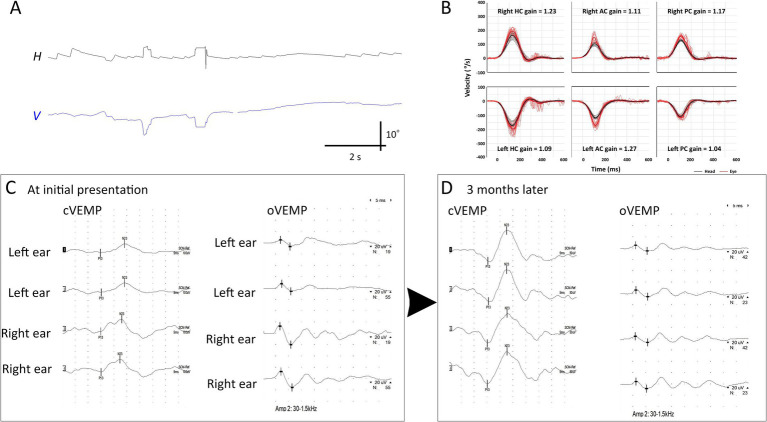
Methods: We retrospectively reviewed the medical records of patients presenting with AVS between September 2019 and April 2024 at a tertiary referral hospital in South Korea. All patients underwent extensive neurotologic evaluation, including cervical and ocular vestibular-evoked myogenic potentials (cVEMP and oVEMP, respectively), subjective visual vertical, video-oculography, video-HITs, caloric tests, and audiometry. Patients also underwent MRI according to a standard protocol for the inner ear and internal acoustic canal with an additional 3D-fluid attenuated inversion recovery sequence acquired 4 h after intravenous gadolinium injection.
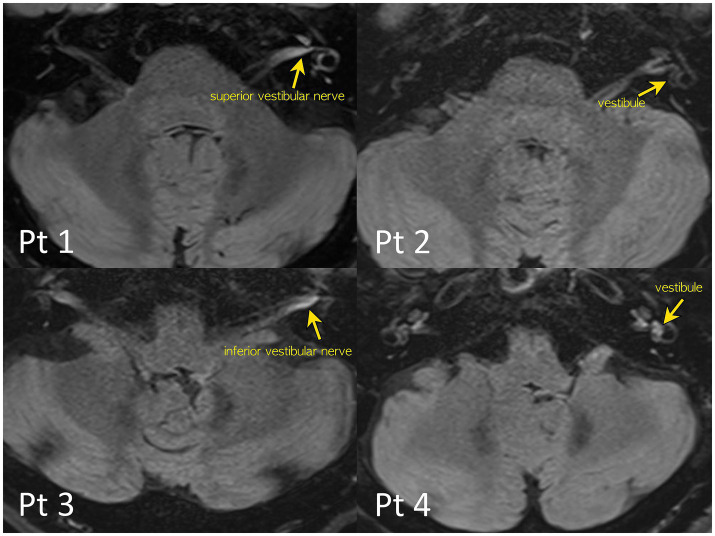
Results: We identified four patients with selective otolith dysfunction. Video-HITs and caloric test results were normal in all patients, except one with a canal paresis on the opposite side of otolithic dysfunction. Patients usually showed abnormal oVEMP (n = 3) and cVEMP (n = 2) or subjective visual vertical (n = 3). Gadolinium enhancements were found in the vestibule (n = 3), inferior (n = 2) or superior (n = 1) vestibular nerves on dedicated inner ear MRI.
Discussion: Selective otolithic dysfunction can present with AVS, which can be easily overlooked. A thorough neurotologic evaluation and MRI dedicated to the inner ear can help detect selective otolithic dysfunction, expanding the clinical spectrum of AVS.
Keywords: dizziness; magnetic resonance imaging; otolith; vertigo; vestibular neuritis.
Copyright © 2024 Kim, Park, Lee, Park, Kim and Kim.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Clinical Features and Neurotologic Findings in Patients With Acute Unilateral Peripheral Vestibulopathy Associated With Antiganglioside Antibody.Neurology. 2023 Nov 7;101(19):e1913-e1921. doi: 10.1212/WNL.0000000000207814. Epub 2023 Sep 25. Neurology. 2023. PMID: 37748887 Free PMC article.
-
[Application of 3D-Flair MRI and vestibular function assessment in profound sudden sensorineural hearing loss patients].Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2025 Jan 7;60(1):2-9. doi: 10.3760/cma.j.cn115330-20240403-00199. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2025. PMID: 39842824 Chinese.
-
Four-hour-delayed 3D-FLAIR MRIs in patients with acute unilateral peripheral vestibulopathy.Ann Clin Transl Neurol. 2024 Aug;11(8):2030-2039. doi: 10.1002/acn3.52123. Epub 2024 Jun 14. Ann Clin Transl Neurol. 2024. PMID: 38874375 Free PMC article.
-
Diagnosing vestibular hypofunction: an update.J Neurol. 2021 Jan;268(1):377-385. doi: 10.1007/s00415-020-10139-4. Epub 2020 Aug 7. J Neurol. 2021. PMID: 32767115 Free PMC article. Review.
-
Isolated vestibular nuclear infarction: report of two cases and review of the literature.J Neurol. 2014 Jan;261(1):121-9. doi: 10.1007/s00415-013-7139-0. Epub 2013 Oct 27. J Neurol. 2014. PMID: 24162036 Review.
References
-
- Brandt T. Otolithic vertigo. Adv Otorhinolaryngol. (2001) 58:34–47. Available at: https://books.google.co.kr/books?hl=en&lr=&id=UjjoxDKygXAC&oi=fnd&pg=PA3... PMID: - PubMed
-
- Murofushi T, Komiyama S, Suizu R, Yoshimura E. Otolithic vertigo in children: report of 3 cases. Acta Oto Laryngol Case Rep. (2016) 1:71–4. doi: 10.1080/23772484.2016.1235466 - DOI
LinkOut - more resources
Full Text Sources
Miscellaneous