

Neurocysticercosis: unwinding the radiological conundrum
- PMID: 39777324
- PMCID: PMC11705042
- DOI: 10.5114/pjr/193968
Neurocysticercosis: unwinding the radiological conundrum
Abstract
Purpose: To study the distinct imaging characteristics of parenchymal neurocysticercosis (NCC) that aid in distinguishing it from other diseases.
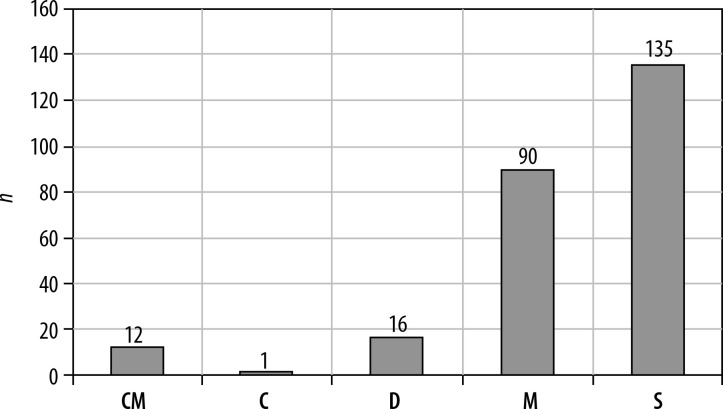
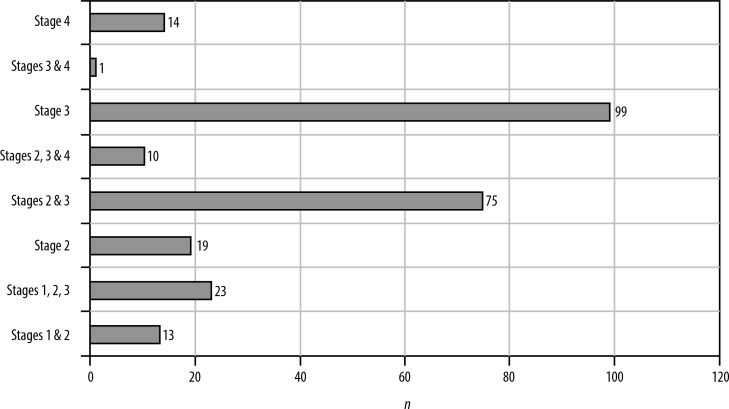
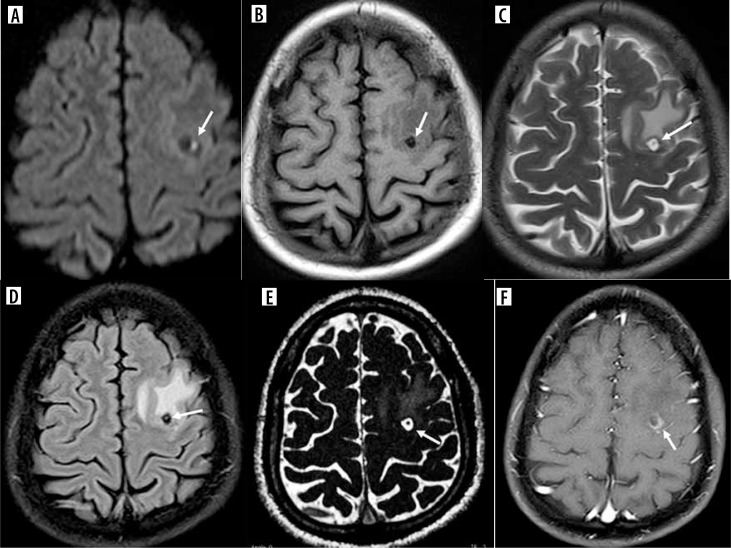
Material and methods: Two hundred fifty patients with NCC were selected based on identification of the scolex. T2 weighted, T1 fluid attenuated inversion recovery (FLAIR), T2 FLAIR, susceptibility weighted imaging, constructive interference in steady state, diffusion weighted imaging, and T1 weighted contrast sequences were performed. The imaging characteristics of the cysts at various stages were analyzed.
Results: This study presents previously undocumented imaging findings of NCC, establishing absolute, major, and minor criteria for its diagnosis based on magnetic resonance imaging features.
Conclusions: Utilizing imaging criteria for diagnosing NCC, as per the study's sequences, can effectively narrow down differential diagnoses and lead to accurate identification.
Keywords: Taenia solium; corona sign; degenerating neurocysticercus cyst; magnetic resonance imaging; neurocysticercosis; scolex.
© Pol J Radiol 2024.
Figures











References
-
- Rajshekhar V. Evolution of concepts in the management of cysticercosis of the brain: Then (1970) and now (2018). Neurol India 2018; 66: 919-927. - PubMed
-
- Tharmalingam J, Prabhakar AT, Gangadaran P, Dorny P, Vercruysse J, Geldhof P, et al. . Host Th1/Th2 immune response to Taenia soliumcyst antigens in relation to cyst burden of neurocysticercosis. Parasite Immunol 2016; 38: 628-634. - PubMed
-
- Arora N, Tripathi S, Sao R, Mondal P, Mishra A, Prasad A. Molecular neuro-pathomechanism of neurocysticercosis: how host genetic factors influence disease susceptibility. Mol Neurobiol 2018; 55: 1019-1025. - PubMed
LinkOut - more resources
Full Text Sources