

Imaging of intramedullary tumours of the spinal cord
- PMID: 39777329
- PMCID: PMC11705043
- DOI: 10.5114/pjr/192424
Imaging of intramedullary tumours of the spinal cord
Abstract
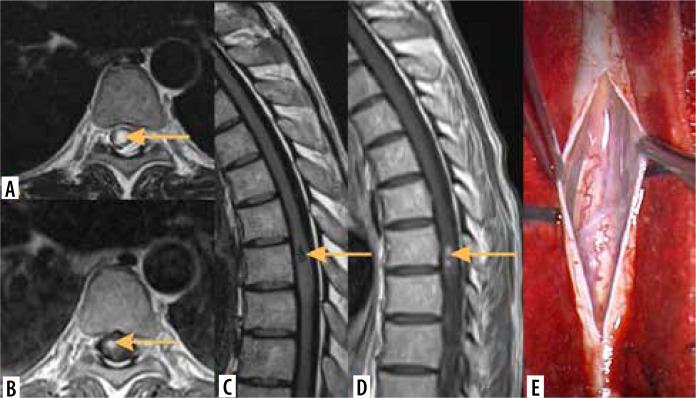
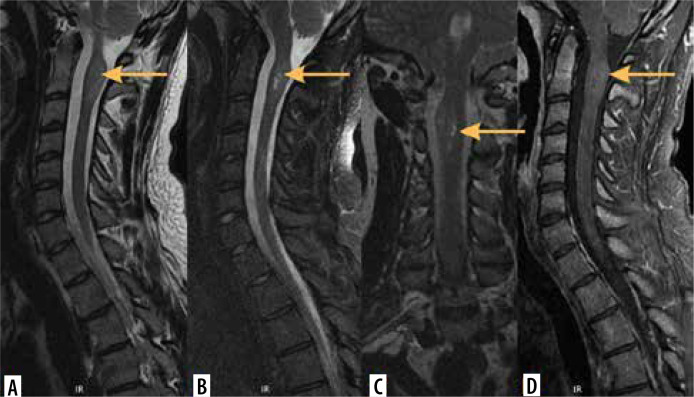
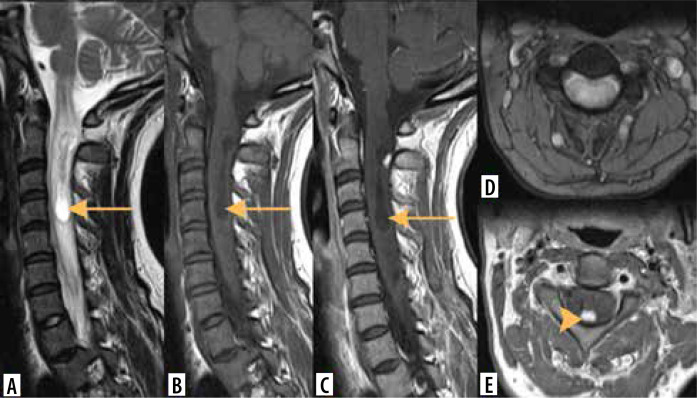
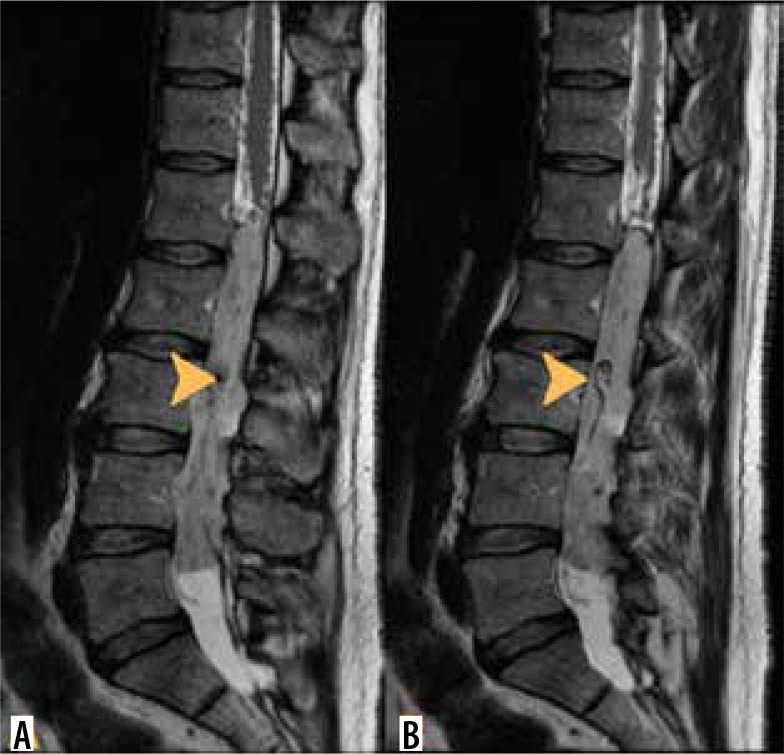
Intramedullary tumours (IMTs) are the least common neoplasms of the spinal canal. The majority of them are ependymomas and astrocytomas, the third commonest is haemangioblastoma, while other tumours of the spinal cord are relatively rare. This review presents on update on the imaging of spinal cord tumours. Magnetic resonance imaging (MRI) is the imaging method of choice in diagnosing IMTs, with other modalities playing a supplementary role. The authors discuss the MRI protocol in IMTs including advanced techniques and present the imaging features of particular tumours. The differentiation of IMTs from other spinal cord diseases is also presented.
Keywords: MRI; intramedullary tumours; spine imaging.
© Pol J Radiol 2024.
Figures






Similar articles
-
Magnetic Resonance Imaging Evaluation of Common Spinal Intramedullary Tumours: Ependymoma and Astrocytoma.Mymensingh Med J. 2023 Jul;32(3):749-756. Mymensingh Med J. 2023. PMID: 37391969
-
Diagnosis of spinal cord ependymoma and astrocytic tumours with magnetic resonance imaging.J Clin Neurosci. 1999 Mar;6(2):128-132. doi: 10.1054/jocn.1997.0005. J Clin Neurosci. 1999. PMID: 10833579
-
Intramedullary tumours and tumour mimics.Clin Radiol. 2020 Nov;75(11):876.e17-876.e32. doi: 10.1016/j.crad.2020.05.010. Epub 2020 Jun 23. Clin Radiol. 2020. PMID: 32591229 Review.
-
Spinal perimedullary vein enlargement sign: an added value for the differentiation between intradural-extramedullary and intramedullary tumors on magnetic resonance imaging.Neuroradiology. 2016 Nov;58(11):1117-1124. doi: 10.1007/s00234-016-1744-4. Epub 2016 Sep 5. Neuroradiology. 2016. PMID: 27596484
-
Conventional and Advanced Imaging of Spinal Cord Tumors.Neuroimaging Clin N Am. 2023 Aug;33(3):389-406. doi: 10.1016/j.nic.2023.03.001. Epub 2023 May 18. Neuroimaging Clin N Am. 2023. PMID: 37356858 Review.
References
-
- Das JM, Hoang S, Mesfin FB. Intramedullary spinal cord tumors. In: StatPearls; Treasure Island, FL: StatPearls Publishing; 2023.
-
- Merhemic Z, Stosic-Opincal T, Thurnher MM. Neuroimaging of spinal tumors. Magn Reson Imaging Clin N Am 2016; 24: 563-579. - PubMed
-
- Pinter NK, Pfiffner TJ, Mechtler LL. Neuroimaging of spine tumors. Handb Clin Neurol 2016; 136: 689-706. - PubMed
-
- Shah LM, Salzman KL. Conventional and advanced imaging of spinal cord tumors. Neuroimaging Clin N Am 2023; 33: 389-406. - PubMed
Publication types
LinkOut - more resources
Full Text Sources