

Establishing reference curves for vital tissue perfusion using quantitative near-infrared fluorescence imaging with indocyanine green
- PMID: 39777554
- PMCID: PMC11706885
- DOI: 10.1007/s00423-024-03589-1
Establishing reference curves for vital tissue perfusion using quantitative near-infrared fluorescence imaging with indocyanine green
Abstract
Purpose: Assessment of tissue perfusion using near-infrared fluorescence (NIR) with indocyanine green (ICG) is gaining popularity, however reliable and objective interpretation remains a challenge. Therefore, this study aimed to establish reference curves for vital tissue perfusion across target tissues using this imaging modality.
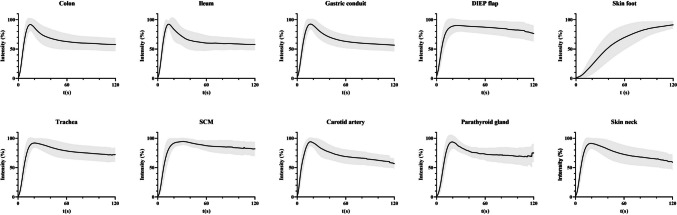
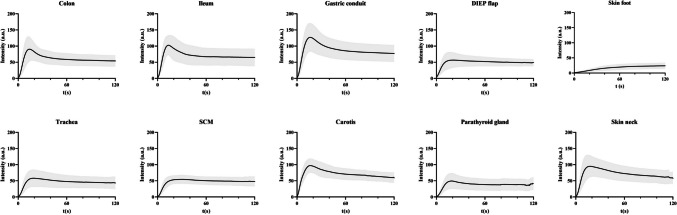
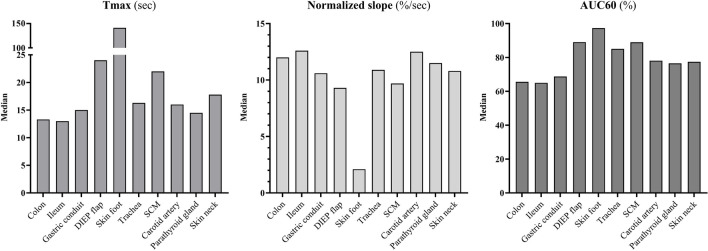
Methods: Data from five prospective study cohorts conducted in three Dutch academic medical centres between December 2018 and June 2023 was included. Quantitative analysis using time-intensity curves was performed in ten target tissues, including the colon, ileum, gastric conduit, deep inferior epigastric artery perforator (DIEP) flap, skin of the foot, trachea, sternocleidomastoid muscle (SCM), carotid artery, parathyroid gland, and skin of the neck.
Results: A total of 178 patients were included in this study, representing 303 target tissues. Three different patterns of reference curves were identified based on a subjective assessment. Seven out of ten tissues showed a reference curve with rapid inflow (median time-to-max (tmax): 13.0-17.8 s, median maximum-normalized-slope (slope norm): 10.6-12.6%/sec), short outflow (median area-under-the-curve of tmax + 60 s (AUC60): 65.0-85.1%) followed by a gradual/absent outflow. Secondly, the DIEP flap and SCM tissue showed a reference curve with longer inflow (median tmax: 24.0, 22.0 s, median slope norm: 9.3, 9.7%/sec respectively) and reduced outflow (median AUC60: 89.1, 89.0% respectively). Thirdly, the skin of the foot showed slow inflow (median tmax 141.1 s, median norm slope 2.1%/sec) without outflow.
Conclusion: This study demonstrates reference curves for vital tissue perfusion of multiple target tissues identified with ICG NIR fluorescence imaging, providing a critical step towards the clinical implementation of this technique.
Keywords: Indocyanine green; Near-infrared fluorescence; Quantification; Surgery; Tissue perfusion.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of Interest: The authors declare no competing interests.
Figures

References
-
- Matienzo D, Bordoni B (2020) Anatomy, blood flow [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
