

Clinical significance of small dense low-density lipoprotein cholesterol measurement in type 2 diabetes
- PMID: 39778086
- PMCID: PMC11871407
- DOI: 10.1111/jdi.14398
Clinical significance of small dense low-density lipoprotein cholesterol measurement in type 2 diabetes
Abstract
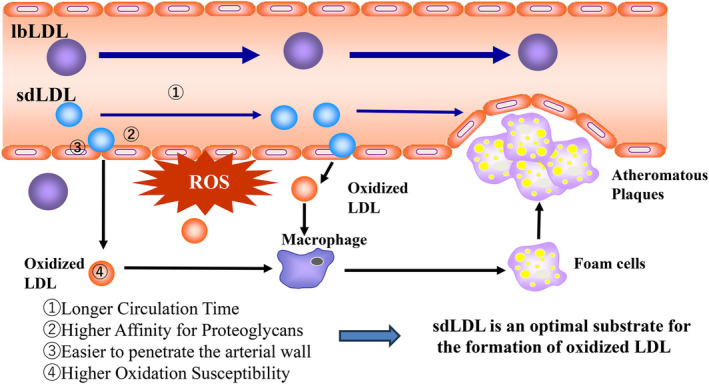
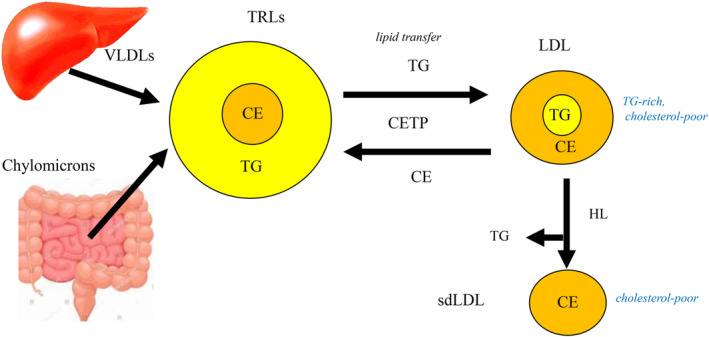
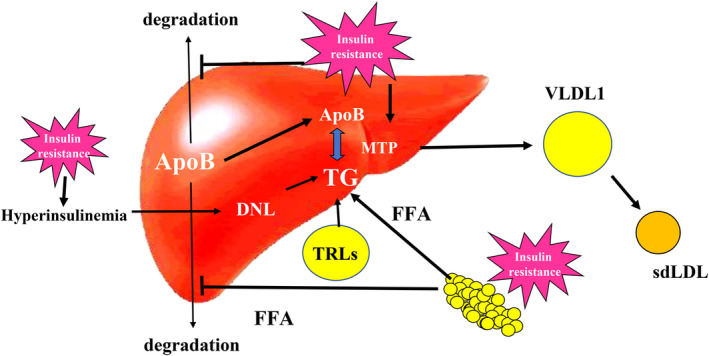
Low-density lipoprotein cholesterol (LDL-C) is known to be a causal substance of atherosclerosis, but its usefulness as a predictive biomarker for atherosclerotic cardiovascular disease (ASCVD) is limited. In patients with type 2 diabetes (T2D), LDL-C concentrations do not markedly increase, while triglycerides (TG) concentrations are usually elevated. Although TG is associated with ASCVD risk, they do not play a direct role in the formation of atheromatous plaques. TG changes the risk of ASCVD in a way that is dependent on LDL-C, and TG is the primary factor in reducing LDL particle size. Small dense (sd)LDL, a potent atherogenic LDL subfraction, best explains the "Atherogenic Duo" of TG and LDL-C. Although hypertriglyceridemia is associated with small-sized LDL, patients with severe hypertriglyceridemia and low LDL-C rarely develop ASCVD. This suggests that quantifying sdLDL is more clinically relevant than measuring LDL size. We developed a full-automated direct sdLDL-C assay, and it was proven that sdLDL-C is a better predictor of ASCVD than LDL-C. The sdLDL-C level is specifically elevated in patients with metabolic syndrome and T2D who have insulin resistance. Due to its clear link to metabolic dysfunction, sdLDL-C could be named "metabolic LDL-C." Insulin resistance/hyperinsulinemia promotes TG production in the liver, causing steatosis and overproduction of VLDL1, a precursor of sdLDL. sdLDL-C is closely associated with steatotic liver disease and chronic kidney disease, which are common complications in T2D. This review focuses on T2D and discusses the clinical significance of sdLDL-C including its composition, pathophysiology, measurements, association with ASCVD, and treatments.
Keywords: Cardiovascular disease; Small dense LDL cholesterol; Triglycerides.
© 2025 The Author(s). Journal of Diabetes Investigation published by Asian Association for the Study of Diabetes (AASD) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
Tsutomu Hirano receives advisory fees from Denka Co., Ltd. and lecture fees from Kowa, Novo Nordisk Pharma, Eli Lilly Japan, and Tanabe Mitsubishi Pharma.
Figures
Similar articles
-
Small Dense Low-Density Lipoprotein Cholesterol Is the Most Atherogenic Lipoprotein Parameter in the Prospective Framingham Offspring Study.J Am Heart Assoc. 2021 Feb;10(5):e019140. doi: 10.1161/JAHA.120.019140. Epub 2021 Feb 15. J Am Heart Assoc. 2021. PMID: 33586462 Free PMC article.
-
Small dense low-density lipoprotein as biomarker in the elderly.Clin Biochem. 2025 Jun;137:110916. doi: 10.1016/j.clinbiochem.2025.110916. Epub 2025 Mar 17. Clin Biochem. 2025. PMID: 40107376
-
Specific Increase in Small Dense Low-Density Lipoprotein-Cholesterol Levels beyond Triglycerides in Patients with Diabetes: Implications for Cardiovascular Risk of MAFLD.J Atheroscler Thromb. 2024 Jan 1;31(1):36-47. doi: 10.5551/jat.64271. Epub 2023 Jul 11. J Atheroscler Thromb. 2024. PMID: 37438123 Free PMC article.
-
[Small-Dense LDL, HDL2, 3].Rinsho Byori. 2016 Jun;64(6):636-642. Rinsho Byori. 2016. PMID: 30695317 Review. Japanese.
-
Small Dense Low-Density Lipoprotein as Biomarker for Atherosclerotic Diseases.Oxid Med Cell Longev. 2017;2017:1273042. doi: 10.1155/2017/1273042. Epub 2017 May 7. Oxid Med Cell Longev. 2017. PMID: 28572872 Free PMC article. Review.
Cited by
-
Unraveling the role of cumulative triglyceride-total cholesterol-body weight index in stroke development: evidence from the CHARLS cohort.Front Med (Lausanne). 2025 Jul 10;12:1616520. doi: 10.3389/fmed.2025.1616520. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40708645 Free PMC article.
-
Relationship of small dense low-density lipoprotein cholesterol level with pre-diabetes and newly detected type 2 diabetes.Sci Rep. 2025 Jun 4;15(1):19500. doi: 10.1038/s41598-025-03133-1. Sci Rep. 2025. PMID: 40461580 Free PMC article.
References
-
- Ference BA, Ginsberg HN, Graham I, et al. Low‐density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European atherosclerosis society consensus panel. Eur Heart J 2017; 38: 2459–2472. - PMC - PubMed
-
- The Expert Panel . Third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III): Final report. Circulation 2002; 106: 3143–3421. - PubMed
-
- Ginsberg HN, Packard CJ, Chapman MJ, et al. Triglyceride‐rich lipoproteins and their remnants: Metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies‐a consensus statement from the European atherosclerosis society. Eur Heart J 2021; 42: 4791–4806. - PMC - PubMed
-
- Miller M, Stone NJ, Ballantyne C, et al. American Heart Association clinical Lipidology, thrombosis, and prevention Committee of the Council on nutrition, physical activity, and metabolism; council on arteriosclerosis, thrombosis and vascular biology; council on cardiovascular nursing; council on the kidney in cardiovascular disease. Triglycerides and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2011; 123: 2292–2333. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
