

GOLD grade-specific characterization of COPD in the COSYCONET multi-center trial: comparison of semiquantitative MRI and quantitative CT
- PMID: 39779513
- PMCID: PMC12165896
- DOI: 10.1007/s00330-024-11269-3
GOLD grade-specific characterization of COPD in the COSYCONET multi-center trial: comparison of semiquantitative MRI and quantitative CT
Abstract
Objectives: We hypothesized that semiquantitative visual scoring of lung MRI is suitable for GOLD-grade specific characterization of parenchymal and airway disease in COPD and that MRI scores correlate with quantitative CT (QCT) and pulmonary function test (PFT) parameters.
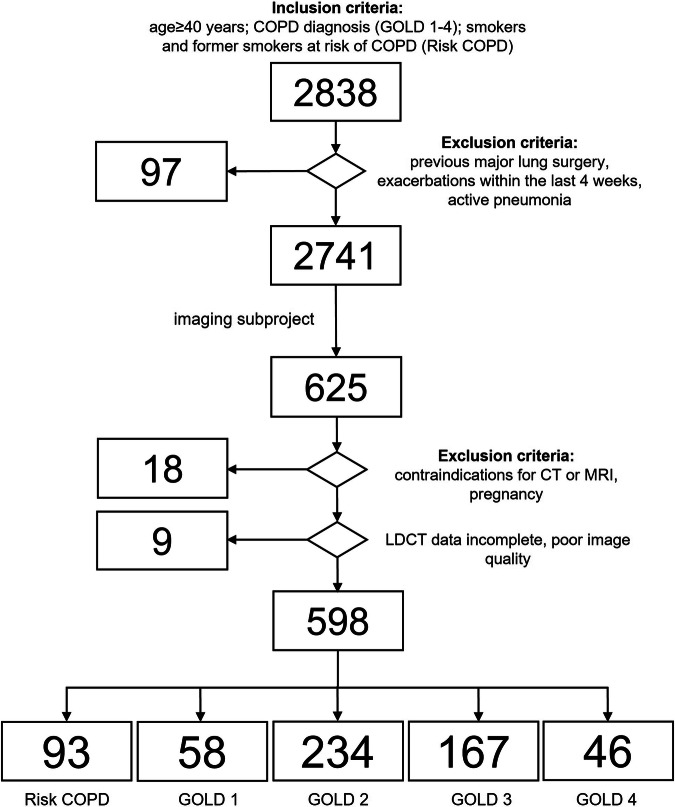
Methods: Five hundred ninety-eight subjects from the COSYCONET study (median age = 67 (60-72)) at risk for COPD or with GOLD1-4 underwent PFT, same-day paired inspiratory/expiratory CT, and structural and contrast-enhanced MRI. QCT assessed total lung volume (TLV), emphysema, and air trapping by parametric response mapping (PRMEmph, PRMfSAD) and airway disease by wall percentage (WP). MRI was analyzed using a semiquantitative visual scoring system for parenchymal defects, perfusion defects, and airway abnormalities. Descriptive statistics, Spearman correlations, and ANOVA analyses were performed.
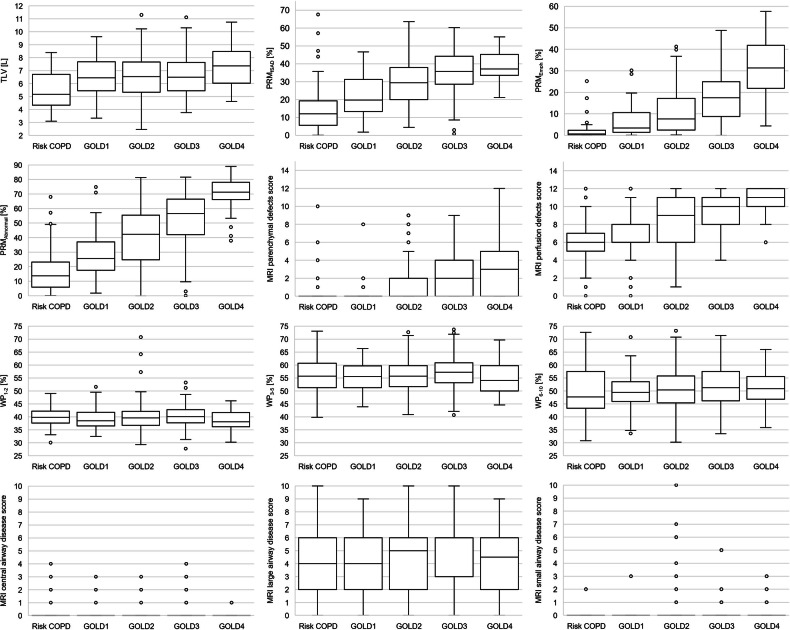
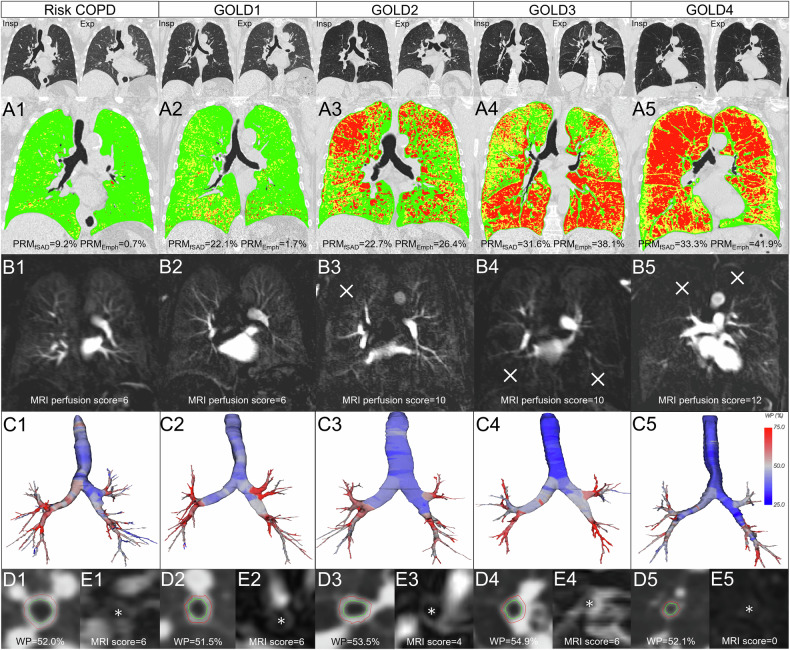
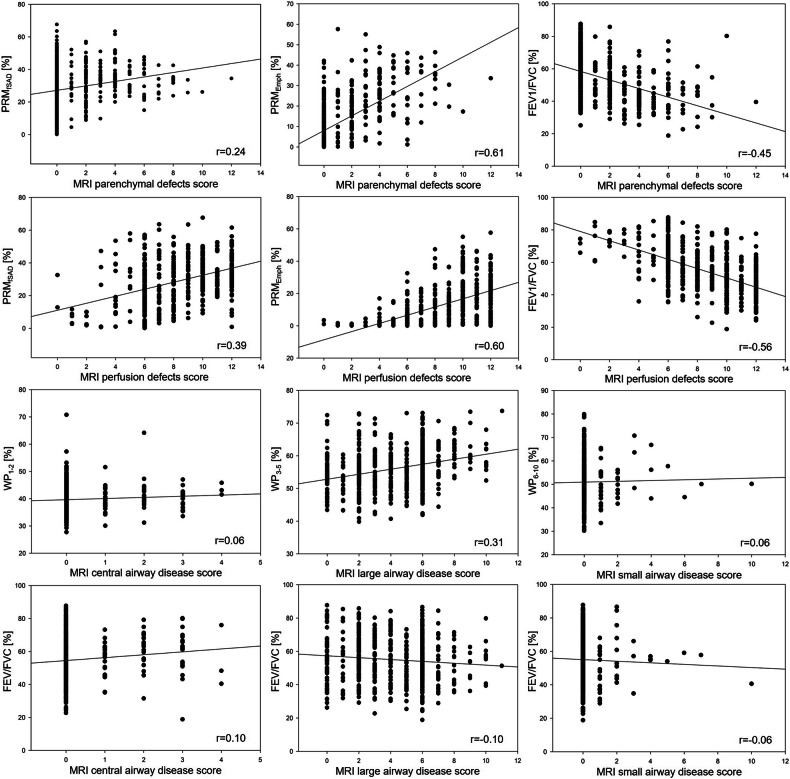
Results: TLV, PRMEmph, and MRI scores for parenchymal and perfusion defects were all higher with each GOLD grade, reflecting the extension of emphysema (all p < 0.001). Airway analysis showed the same trends with higher WP and higher MRI large airway disease scores in GOLD3 and lower WP and MRI scores in GOLD4 (p = 0.236 and p < 0.001). Regional heterogeneity was less evident on MRI, while PRMEmph and MRI perfusion defect scores were higher in the upper lobes, and WP and MRI large airway disease scores were higher in the lower lobes. MRI parenchymal and perfusion scores correlated moderately with PRMEmph (r = 0.61 and r = 0.60) and moderately with FEV1/FVC (r = -0.56).
Conclusion: Multi-center semiquantitative MRI assessments of parenchymal and airway disease in COPD matched GOLD grade-specific imaging features on QCT and detected regional disease heterogeneity. MRI parenchymal disease scores were correlated with QCT and lung function parameters.
Key points: Question Do MRI-based scores correlate with QCT and PFT parameters for GOLD-grade specific disease characterization of COPD? Findings MRI can visualize the parenchymal and airway disease features of COPD. Clinical relevance Lung MRI is suitable for GOLD-grade specific disease characterization of COPD and may serve as a radiation-free imaging modality in scientific and clinical settings, given careful consideration of its potential and limitations.
Keywords: Chronic obstructive pulmonary disease; Computed tomography; Magnetic resonance imaging; Pulmonary emphysema.
© 2025. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is Philip Konietzke. Conflict of interest: P.K. has no relevant relationships. O.W. airway analysis technology is licensed to Imbio, LLC. S.M.F.T. has no relevant relationships. S.N. has no relevant relationships. F.W. has no relevant relationships. M.K. employee at Boehringer Ingelheim. B.J.J. has no relevant relationships. C.F.V. grants or contracts from the German Ministry of Education and Science (BMBF), AstraZeneca, Boehringer Ingelheim, Grifols, GlaxoSmithKline, and Novartis; consulting fees from Aerogen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Nuvaira; payment or honoraria for lectures/presentations from Aerogen, AstraZeneca, Boehringer Ingelheim. R.A.J. has no relevant relationships. H.-U.K. Bayer provided consumables to the consortium; the institution receives payment from Siemens, Philips, and Boehringer Ingelheim; consulting fees to the author from Median; and payment or honoraria for lectures/presentations to the author from Siemens, Philips, Boehringer Ingelheim, MSD, and Sanofi. C.P.H. grants/contracts from Siemens (2012–2014), Pfizer (2012–2014), MeVis (2012, 2013), Boehringer Ingelheim (2014), and German Center for Lung Research (2011ff); consulting fees from Schering-Plough (2009 and 2010), Pfizer (2008–2014), Basilea (2008, 2009, and 2010), Boehringer Ingelheim (2010–2014), Novartis (2010, 2012, and 2014), Roche (2010), Astellas (2011 and 2012), Gilead (2011–2015), MSD (2011–2013), Lilly (2011), Intermune (2013–2014), and Fresenius (2013 and 2014); lecture fees from Gilead (2008–2014), Essex (2008, 2009, and 2010), Schering-Plough (2008, 2009, and 2010), AstraZeneca (2008–2014 and 2022), Lilly (2008, 2009, and 2012), Roche (2008 and 2009), MSD (2009–2014), Pfizer (2010–2014), Bracco (2010 and 2011), MEDA Pharma (2011), Intermune (2011–2014), Chiesi (2012), Siemens (2012), Covidien (2012), Pierre Fabre (2012), Boehringer Ingelheim (2012, 2013, and 2022), Grifols (2012), Novartis (2013–2016), Basilea (2015 and 2016), and Bayer (2016); patent: Method and Device For Representing the Microstructure of the Lungs. IPC8 Class: AA61B5055FI, PAN: 20080208038, Inventors: W Schreiber, U Wolf, AW Scholz, C.P.H.; participation on a data safety monitoring board or advisory board: Schering-Plough (2009 and 2010), Pfizer (2008–2014), Basilea (2008, 2009, and 2010), Boehringer Ingelheim (2010–2014, 2022ff), Novartis (2010, 2012, and 2014), Roche (2010), Astellas (2011 and 2012), Gilead (2011–2015), MSD (2011–2013), Lilly (2011), Intermune (2013–2014), Fresenius (2013 and 2014); leadership or fiduciary roles: chest working group of the German Roentgen Society (national guidelines: bronchial carcinoma, mesothelioma, COPD, screening for bronchial carcinoma, CT and MRI of the chest, pneumonia); consultant of ECIL-3, ECCMID, EORTC/MSG (guideline for diagnosis of infections in immunocompromised hosts); founding member of the working team in infections in immunocompromised hosts of the German Society of Hematology/Oncology (guideline for diagnosis of infections in immunocompromised hosts); faculty member of European Society of Thoracic Radiology (ESTI), European Respiratory Society (ERS), and member in EIBALL (European Imaging Biomarkers Alliance); editor of Medizinische Klinik, Intensivmedizin und Notfallmedizin at Springer publishing; stock/stock options GSK. B.J.J. has no relevant relationships. M.O.W. Bayer provided contrast material for MRI examinations; study grants were paid to institutions from Vertex Pharmaceuticals and Boehringer Ingelheim; and consultancy fees were paid to institutions from Vertex Pharmaceuticals and Boehringer Ingelheim. J.B. Siemens Healthineers helped with MRI protocol design; Bayer provided contrast material used in the study; payment for honorarium for presentation at a workshop from Roche, Boehringer Ingelheim, and Fuji; and president of the European Society of Thoracic Imaging 2022–2023. Statistics and biometry: No complex statistical methods were necessary for this paper. Informed consent: Written informed consent was obtained from all subjects (patients) in this study. Ethical approval: Institutional ethics committee approval was obtained (Ethik-Kommission der Medizinischen Fakultät der Universität Heidelberg, S-656/2012) and all subjects gave their written informed consent prior to the study conduct. Study subjects or cohorts overlap: Some study subjects or cohorts have been previously reported in https://doi.org/10.1007/s00330-024-10610-0 (Phenotyping of COPD with MRI in comparison to same-day CT in a multi-center trial) and “COPD phenotyping based on QCT” (under review). Methodology: Prospective Observational Multicenter study
Figures
References
-
- Coxson HO, Leipsic J, Parraga G, Sin DD (2014) Using pulmonary imaging to move chronic obstructive pulmonary disease beyond FEV1. Am J Respir Crit Care Med 190:135–144 - PubMed
-
- Gould GA, MacNee W, McLean A et al (1988) CT measurements of lung density in life can quantitate distal airspace enlargement—an essential defining feature of human emphysema. Am Rev Respir Dis 137:380–392 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
