

Diet-wide analyses for risk of colorectal cancer: prospective study of 12,251 incident cases among 542,778 women in the UK
- PMID: 39779669
- PMCID: PMC11711514
- DOI: 10.1038/s41467-024-55219-5
Diet-wide analyses for risk of colorectal cancer: prospective study of 12,251 incident cases among 542,778 women in the UK
Abstract
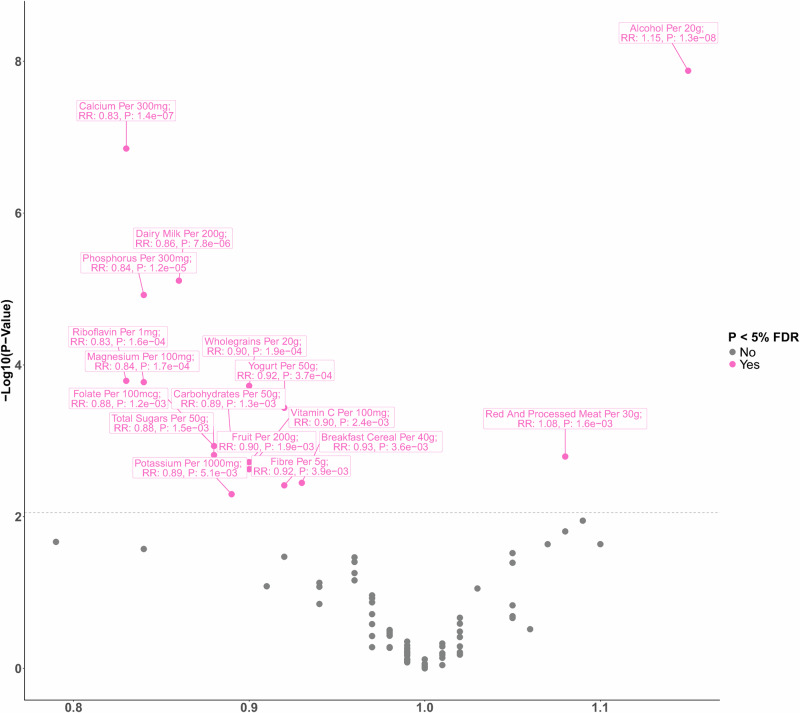
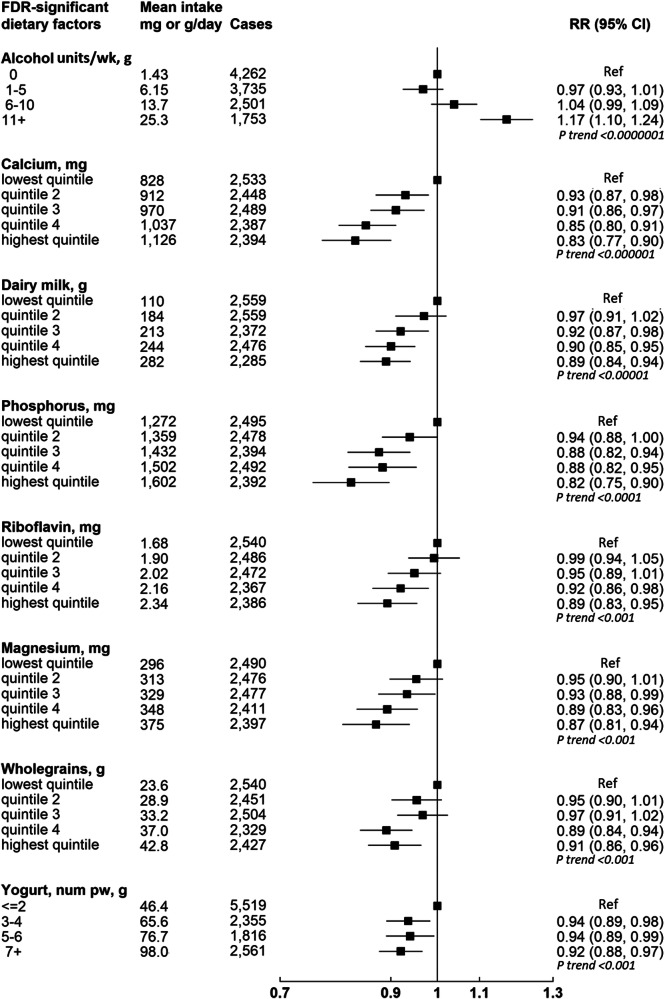
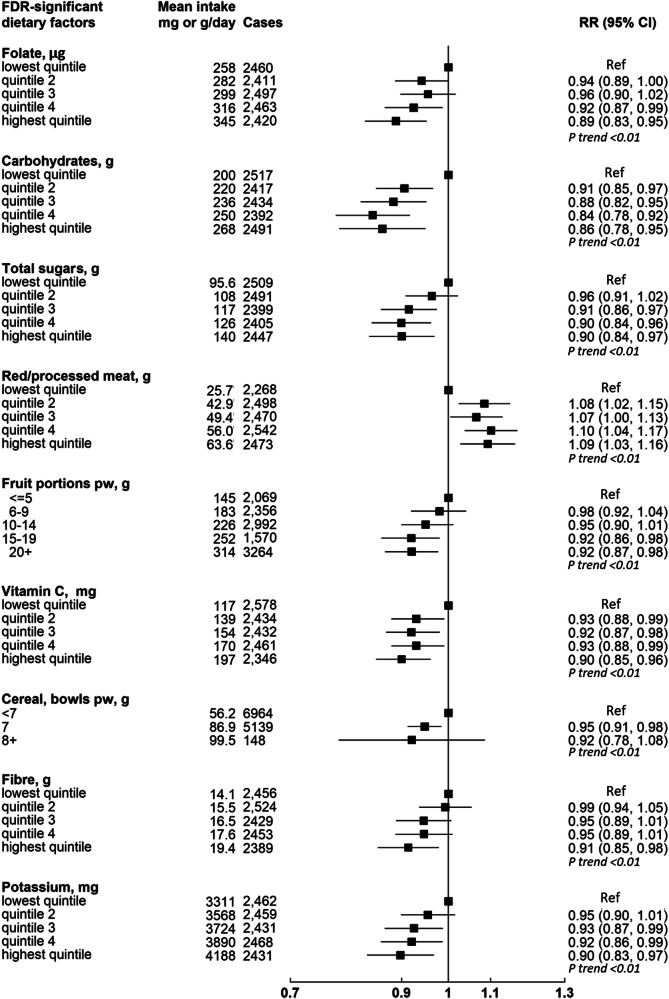
Uncertainty remains regarding the role of diet in colorectal cancer development. We examined associations of 97 dietary factors with colorectal cancer risk in 542,778 Million Women Study participants (12,251 incident cases over 16.6 years), and conducted a targeted genetic analysis in the ColoRectal Transdisciplinary Study, Colon Cancer Family Registry, and Genetics and Epidemiology of Colorectal Cancer Consortium (GECCO). Alcohol (relative risk per 20 g/day=1.15, 95% confidence interval 1.09-1.20) and calcium (per 300 mg/day=0.83, 0.77-0.89) intakes had the strongest associations, followed by six dairy-related factors associated with calcium. We showed a positive association with red and processed meat intake and weaker inverse associations with breakfast cereal, fruit, wholegrains, carbohydrates, fibre, total sugars, folate, and vitamin C. Genetically predicted milk consumption was inversely associated with risk of colorectal, colon, and rectal cancers. We conclude that dairy products help protect against colorectal cancer, and that this is driven largely or wholly by calcium.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: UP was a consultant with AbbVie and her husband is holding individual stocks for the following companies: BioNTech SE – ADR, Amazon, CureVac BV, NanoString Technologies, Google/Alphabet Inc Class C, NVIDIA Corp, Microsoft Corp. The remaining authors declare no competing interests.
Figures
References
-
- Globocan. Cancer Today. Cancer Fact sheets: Colorectal cancer. Absolute numbers, Incidence, Both sexes, in 2022, <http://gco.iarc.fr/today/data/factsheets/cancers/10_8_9-Colorectum-fact-...> (2022).
-
- Globocan. Cancer Over time. Cancer Fact sheets: Colorectal cancer. Age-standardized rate (World) per 100 000, incidence, males and females, (2022).
-
- World Cancer Research Fund & American Institute for Cancer Research. Diet, Nutrition, Physical Activity, and the Prevention of Colorectal Cancer., (2018).
-
- Papadimitriou, N. et al. A Prospective Diet-Wide Association Study for Risk of Colorectal Cancer in EPIC. Clin. Gastroenterol. Hepatol.10.1016/j.cgh.2021.04.028 (2021). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
