

Explainable artificial intelligence to identify follicles that optimize clinical outcomes during assisted conception
- PMID: 39779682
- PMCID: PMC11711444
- DOI: 10.1038/s41467-024-55301-y
Explainable artificial intelligence to identify follicles that optimize clinical outcomes during assisted conception
Abstract
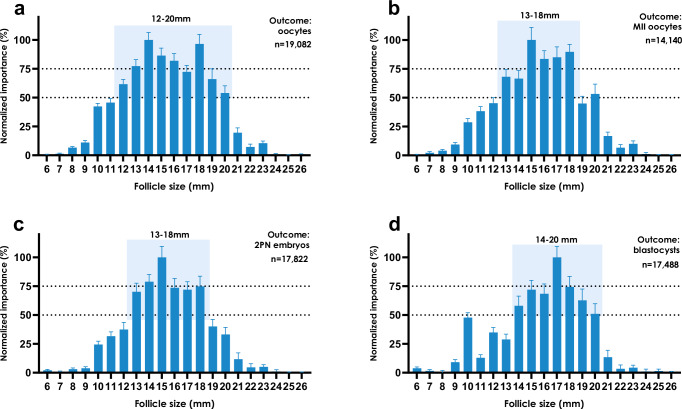
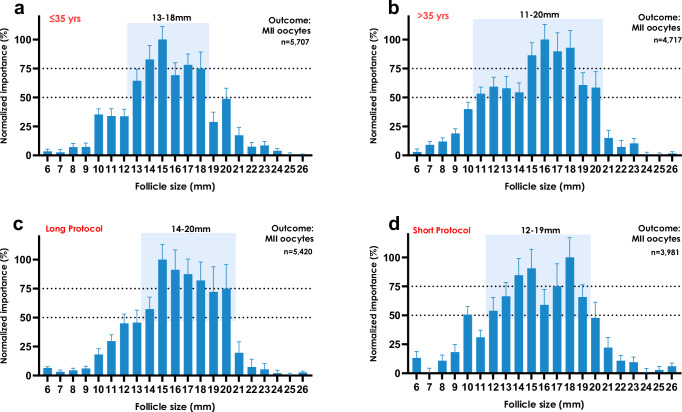
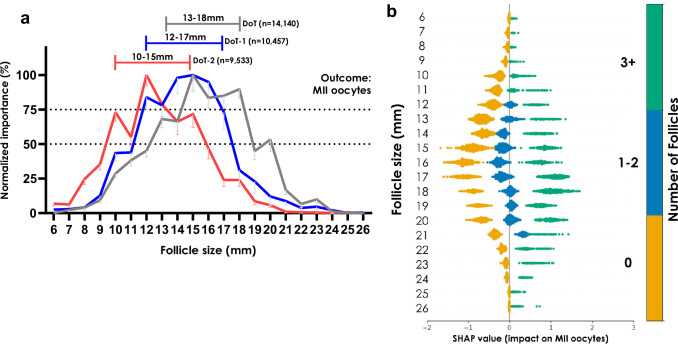
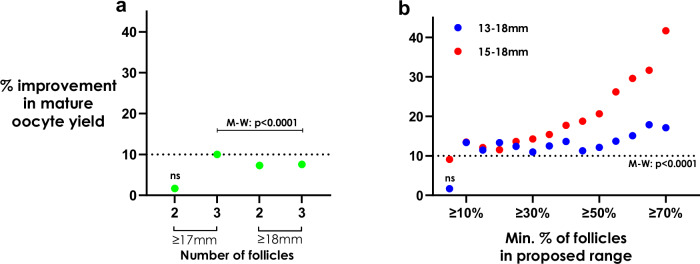
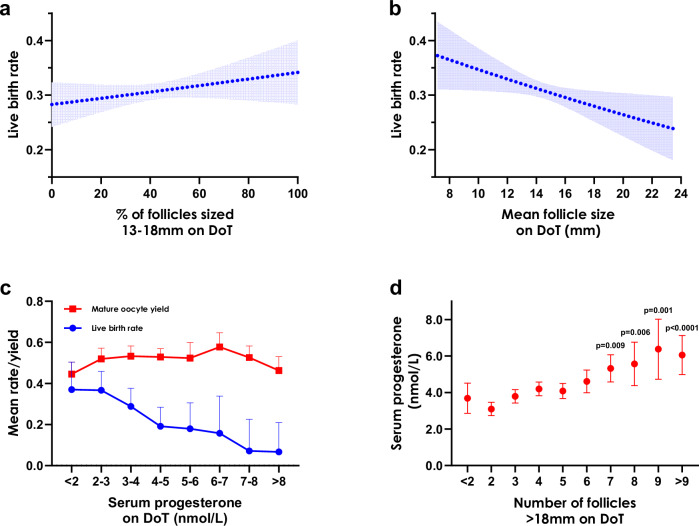
Infertility affects one-in-six couples, often necessitating in vitro fertilization treatment (IVF). IVF generates complex data, which can challenge the utilization of the full richness of data during decision-making, leading to reliance on simple 'rules-of-thumb'. Machine learning techniques are well-suited to analyzing complex data to provide data-driven recommendations to improve decision-making. In this multi-center study (n = 19,082 treatment-naive female patients), including 11 European IVF centers, we harnessed explainable artificial intelligence to identify follicle sizes that contribute most to relevant downstream clinical outcomes. We found that intermediately-sized follicles were most important to the number of mature oocytes subsequently retrieved. Maximizing this proportion of follicles by the end of ovarian stimulation was associated with improved live birth rates. Our data suggests that larger mean follicle sizes, especially those >18 mm, were associated with premature progesterone elevation by the end of ovarian stimulation and a negative impact on live birth rates with fresh embryo transfer. These data highlight the potential of computer technologies to aid in the personalization of IVF to optimize clinical outcomes pending future prospective validation.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: S.H. provides consultancy services for Impli Limited. S.M.N. received grants from NIHR, CSO, and Wellbeing of Women; provided consultancy services for Access Fertility, Ferring Pharmaceuticals, Roche, Ro, and TFP; received honoraria from Ferring Pharmaceuticals, Merck, and Roche; received support for attending meetings and/or travel from Ferring Pharmaceuticals, Merck, and Gideon Richter; and leadership role in the HFEA. W.S.D. received grants from NIHR, MRC, and Imperial Health Charity, and is a consultant for Myovant Sciences Ltd. A.A. has received grants from the BRC; has provided consulting services for Myovant Sciences Ltd; and received support for travel from Merck. The remaining authors declare no competing interests.
Figures
References
-
- Ectors, F. et al. Relationship of human follicular diameter with oocyte fertilization and development after in-vitro fertilization or intracytoplasmic sperm injection. Hum. Reprod.12, 2002–2005 (1997). - PubMed
-
- Shapiro, B. S. et al. The effect of ovarian follicle size on oocyte and embryology outcomes. Fertil. Steril.117, 1170–1176 (2022). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
