

Decreased impulsiveness and MEG normalization after AI-digital therapy in ADHD children: a RCT
- PMID: 39779908
- PMCID: PMC11711623
- DOI: 10.1038/s44184-024-00111-9
Decreased impulsiveness and MEG normalization after AI-digital therapy in ADHD children: a RCT
Abstract
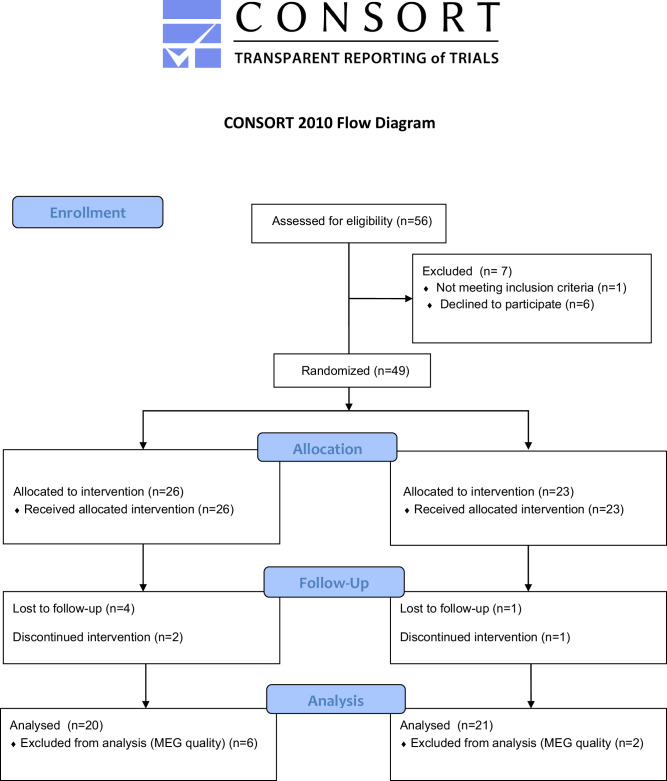
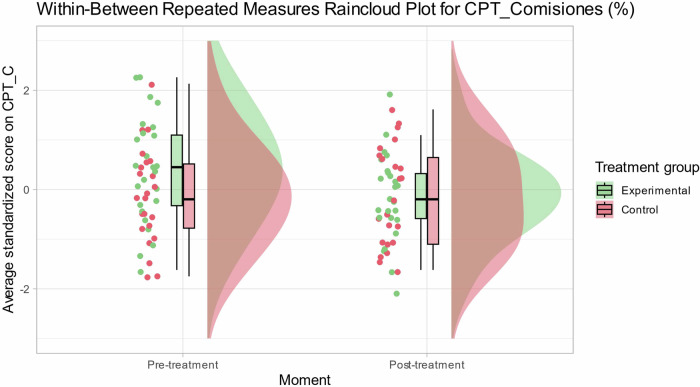
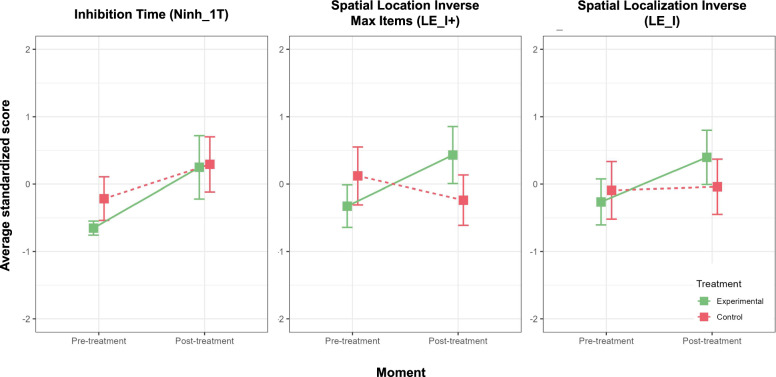
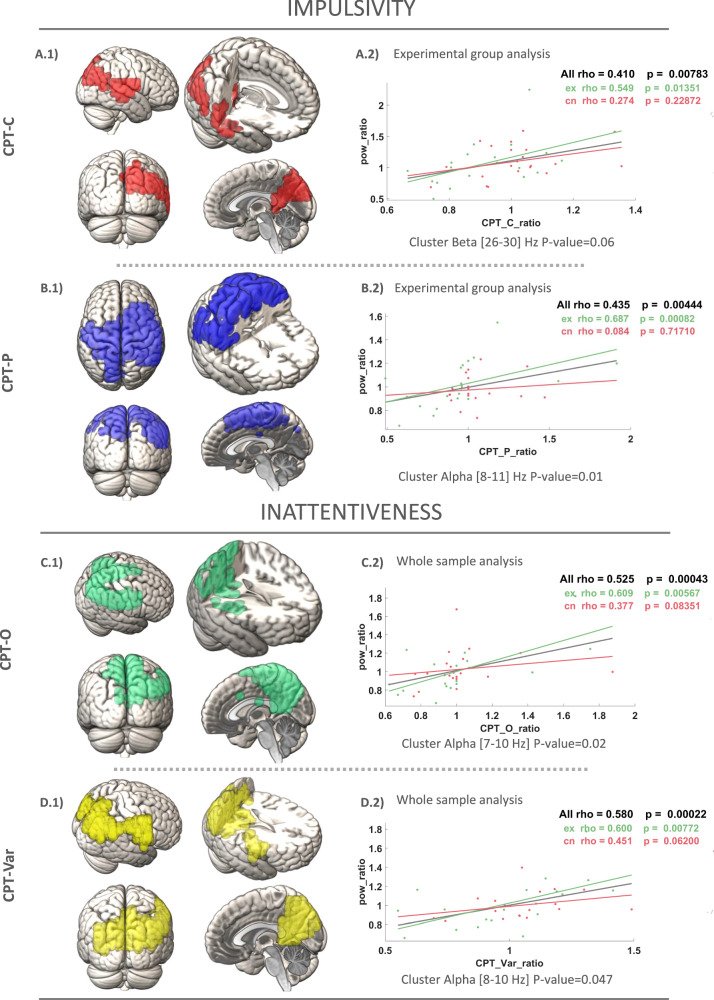
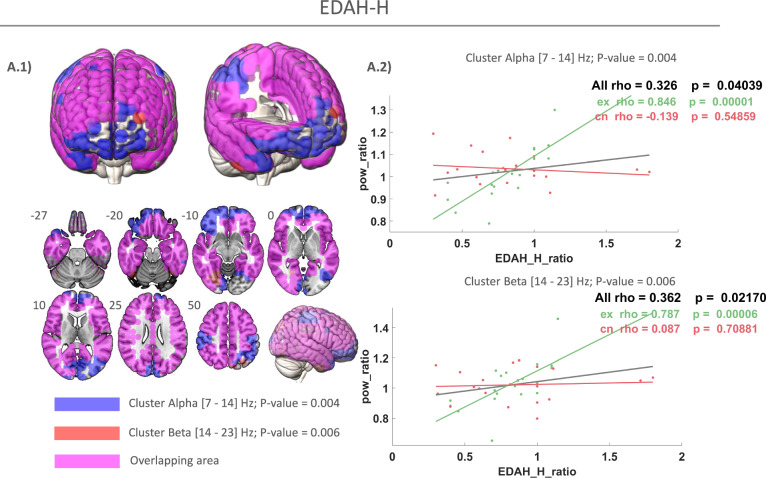
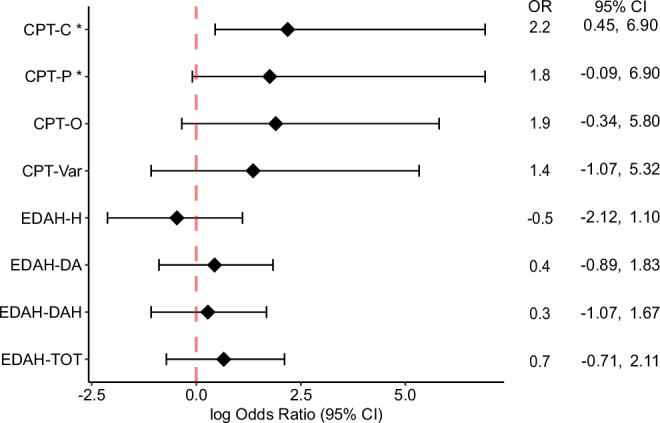
Attention-deficit/hyperactivity disorder (ADHD) presents with symptoms like impulsiveness, inattention, and hyperactivity, often affecting children's academic and social functioning. Non-pharmacological interventions, such as digital cognitive therapy, are emerging as complementary treatments for ADHD. The randomized controlled trial explored the impact of an AI-driven digital cognitive program on impulsiveness, inattentiveness, and neurophysiological markers in 41 children aged 8-12 with ADHD. Participants received either 12 weeks of AI-driven therapy or a placebo intervention. Assessments were conducted pre- and post-intervention and magnetoencephalography (MEG) analyzed brain activity. Results showed significant reductions in impulsiveness and inattentiveness scores in the treatment group, associated with normalized MEG spectral profiles, indicating neuromaturation. Notably, improvements in inhibitory control correlated with spectral profile normalization in the parieto-temporal cortex. Improvements in inhibitory control, linked to normalized spectral profiles, suggest AI-driven digital cognitive therapy can reduce impulsiveness in ADHD children by enhancing neurophysiological efficiency. This emphasizes personalized, technology-driven ADHD treatment, using neurophysiological markers for assessing efficacy.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
A Digital Cognitive-Physical Intervention for Attention-Deficit/Hyperactivity Disorder: Randomized Controlled Trial.J Med Internet Res. 2024 May 10;26:e55569. doi: 10.2196/55569. J Med Internet Res. 2024. PMID: 38728075 Free PMC article. Clinical Trial.
-
A Phase III, Randomized, Double-Blind, Placebo-Controlled Trial Assessing the Efficacy and Safety of Viloxazine Extended-Release Capsules in Adults with Attention-Deficit/Hyperactivity Disorder.CNS Drugs. 2022 Aug;36(8):897-915. doi: 10.1007/s40263-022-00938-w. Epub 2022 Jul 27. CNS Drugs. 2022. PMID: 35896943 Free PMC article. Clinical Trial.
-
Electrophysiological Brain Changes Associated With Cognitive Improvement in a Pediatric Attention Deficit Hyperactivity Disorder Digital Artificial Intelligence-Driven Intervention: Randomized Controlled Trial.J Med Internet Res. 2021 Nov 26;23(11):e25466. doi: 10.2196/25466. J Med Internet Res. 2021. PMID: 34842533 Free PMC article. Clinical Trial.
-
Immediate-release methylphenidate for attention deficit hyperactivity disorder (ADHD) in adults.Cochrane Database Syst Rev. 2021 Jan 18;1(1):CD013011. doi: 10.1002/14651858.CD013011.pub2. Cochrane Database Syst Rev. 2021. PMID: 33460048 Free PMC article.
-
The Role of Physical Activity in ADHD Management: Diagnostic, Digital and Non-Digital Interventions, and Lifespan Considerations.Children (Basel). 2025 Mar 7;12(3):338. doi: 10.3390/children12030338. Children (Basel). 2025. PMID: 40150619 Free PMC article. Review.
Cited by
-
Effects of digital interventions on neuroplasticity and brain function of individuals with developmental disabilities: A systematic review.Internet Interv. 2025 Jul 2;41:100850. doi: 10.1016/j.invent.2025.100850. eCollection 2025 Sep. Internet Interv. 2025. PMID: 40687196 Free PMC article. Review.
References
-
- Sayal, K., Prasad, V., Daley, D., Ford, T. & Coghill, D. ADHD in children and young people: prevalence, care pathways, and service provision. Lancet Psychiatry5, 175–186 (2018). - PubMed
-
- Sibley, M. H., Mitchell, J. T. & Becker, S. P. Method of adult diagnosis influences estimated persistence of childhood ADHD: a systematic review of longitudinal studies. Lancet Psychiatry3, 1157–1165 (2016). - PubMed
-
- Polanczyk, G., De Lima, M. S., Horta, B. L., Biederman, J. & Rohde, L. A. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am. J. Psychiatry164, 942–948 (2007). - PubMed
LinkOut - more resources
Full Text Sources
