

Diagnostic value of the MZXBTCH scoring system for acute complex appendicitis
- PMID: 39779995
- PMCID: PMC11711385
- DOI: 10.1038/s41598-025-85791-9
Diagnostic value of the MZXBTCH scoring system for acute complex appendicitis
Abstract
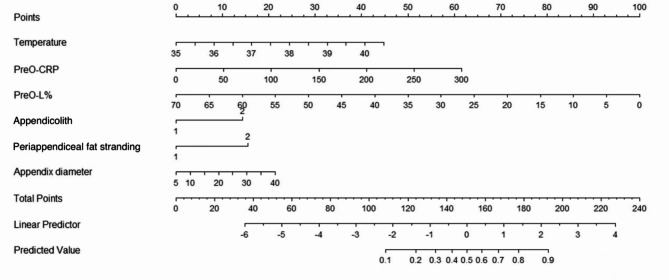
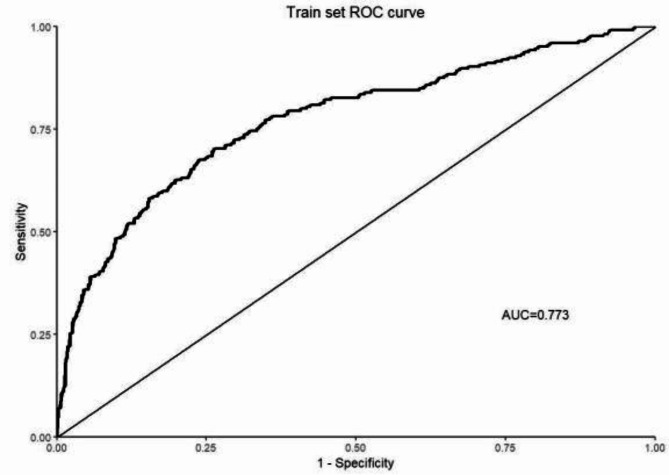
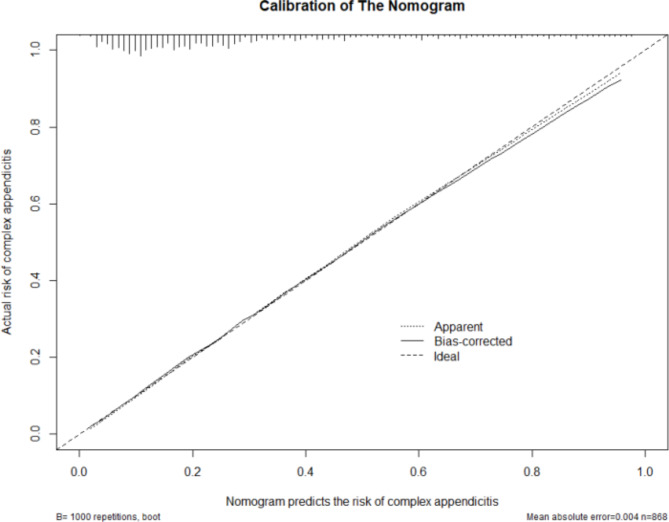
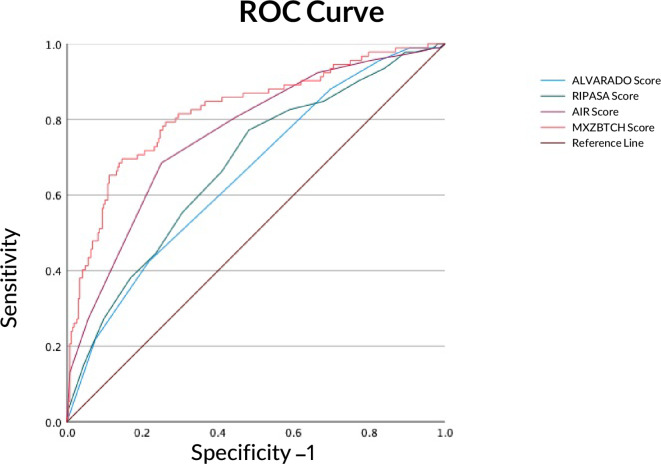
The objective of this study was to develop a novel scoring model, assess its diagnostic value for complex appendicitis, and compare it with existing scoring systems. A total of 1,241 patients with acute appendicitis were included, comprising 868 patients in the modeling group (mean age, 35.6 ± 14.2 years; 52.4% men) and 373 patients in the validation group (mean age, 36.2 ± 13.8 years; 53.1% men). Among them, 28.4% (346/1,241) were diagnosed with complex appendicitis. The distribution of clinical features, laboratory results, and imaging findings was comparable between the two groups. The data from the modeling group were used to develop the MZXBTCH scoring system, which subsequently validated using the validation group data. Based on postoperative pathological diagnoses, the validation group (n = 373) was scored using the Alvarado, Raja Isteri Pengiran Anak Saleha (RIPASA), Appendicitis Inflammatory Response (AIR), and MZXBTCH scoring systems. Receiver operating characteristic (ROC) curves were plotted to compare the diagnostic efficacy of these scoring systems for complex appendicitis. Multivariate logistic regression analysis identified preoperative body temperature (odds ratio (OR) = 1.104; 95% confidence interval (CI) 1.067-1.143; P < 0.001), preoperative C-reactive protein (CRP) level (OR = 1.002; 95% CI 1.001-1.002; P < 0.001), lymphocyte percentage (OR = 0.994; 95% CI 0.990-0.996; P < 0.001), appendiceal fecal stones (OR = 1.127; 95% CI 1.068-1.190; P < 0.001), periappendiceal fat stranding (OR = 1.133; 95% CI 1.072-1.198; P < 0.001), and appendix diameter (OR = 1.013; 95% CI 1.004-1.022; P < 0.001) as independent risk factors for complex appendicitis. Using R programming, a nomogram based on these independent risk factors was constructed to derive MZXBTCH scores. ROC curve analysis of the MZXBTCH model indicated an area under the curve (AUC) of 0.773. ROC curve analysis revealed that the AUC values of the Alvarado, RIPASA, AIR, and MZXBTCH scoring systems were 0.66, 0.68, 0.76, and 0.82, respectively. Sensitivities were 64.29%, 66.33%, 68.37%, and 74.49%, and specificities were 55.64%, 60%, 75.64%, and 76.36%, respectively. Positive predictive values were 0.34, 0.37, 0.5, and 0.53, while negative predictive values were 0.81, 0.83, 0.87, and 0.89. Accuracy rates were 0.58, 0.62, 0.74, and 0.76, respectively. The MZXBTCH scoring system demonstrated higher sensitivity, specificity, and accuracy compared with the Alvarado, RIPASA, and AIR scoring systems in distinguishing complex appendicitis.
Keywords: Complex appendicitis; Diagnosis, nomogram; MZXBTCH scoring system.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: This study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethical approval was waived by the Ethics Committee of Tsinghua Changgung Hospital due to the retrospective nature of the study. Written informed consent was waived due to the retrospective nature of this study by the Ethics Committee of Tsinghua Changgung Hospital.
Figures
Similar articles
-
Comparison of Raja Isteri Pengiran Anak Saleha Appendicitis and modified Alvarado scoring systems in the diagnosis of acute appendicitis.ANZ J Surg. 2020 Apr;90(4):521-524. doi: 10.1111/ans.15607. Epub 2019 Dec 15. ANZ J Surg. 2020. PMID: 31840385
-
A Comparative Study of Raja Isteri Pengiran Anak Saleha and Alvarado Scores to Diagnose Acute Appendicitis.J Nepal Health Res Counc. 2021 Apr 23;19(1):111-114. doi: 10.33314/jnhrc.v19i1.1435. J Nepal Health Res Counc. 2021. PMID: 33934144
-
RIPASA and air scoring systems are superior to alvarado scoring in acute appendicitis: Diagnostic accuracy study.Ann Med Surg (Lond). 2020 Sep 24;59:138-142. doi: 10.1016/j.amsu.2020.09.029. eCollection 2020 Nov. Ann Med Surg (Lond). 2020. PMID: 33024555 Free PMC article.
-
Alvarado or RIPASA score for diagnosis of acute appendicitis? A meta-analysis of randomized trials.Int J Surg. 2018 Aug;56:307-314. doi: 10.1016/j.ijsu.2018.07.003. Epub 2018 Jul 12. Int J Surg. 2018. PMID: 30017607 Review.
-
Comparison of RIPASA and ALVARADO scores for risk assessment of acute appendicitis: A systematic review and meta-analysis.PLoS One. 2022 Sep 30;17(9):e0275427. doi: 10.1371/journal.pone.0275427. eCollection 2022. PLoS One. 2022. PMID: 36178953 Free PMC article.
References
-
- Wickramasinghe, D. P., Xavier, C. & Samarasekera, D. N. The Worldwide Epidemiology of Acute Appendicitis: an analysis of the Global Health Data Exchange Dataset. World J. Surg.45, 1999–2008 (2021). - PubMed
-
- Liang, D. et al. Development and validation of a deep learning and Radiomics Combined Model forDifferentiating complicated from uncomplicated Acute Appendicitis. Acad. Radiol. (2023). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
