

The role of the left primary motor cortex in apraxia
- PMID: 39780250
- PMCID: PMC11716253
- DOI: 10.1186/s42466-024-00359-8
The role of the left primary motor cortex in apraxia
Abstract
Background: Apraxia is a motor-cognitive disorder that primary sensorimotor deficits cannot solely explain. Previous research in stroke patients has focused on damage to the fronto-parietal praxis networks in the left hemisphere (LH) as the cause of apraxic deficits. In contrast, the potential role of the (left) primary motor cortex (M1) has largely been neglected. However, recent brain stimulation and lesion-mapping studies suggest an involvement of left M1 in motor cognitive processes-over and above its role in motor execution. Therefore, this study explored whether the left M1 plays a specific role in apraxia.
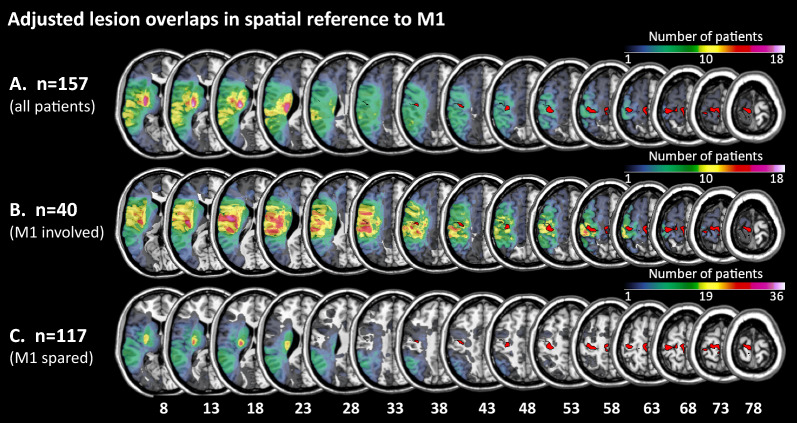
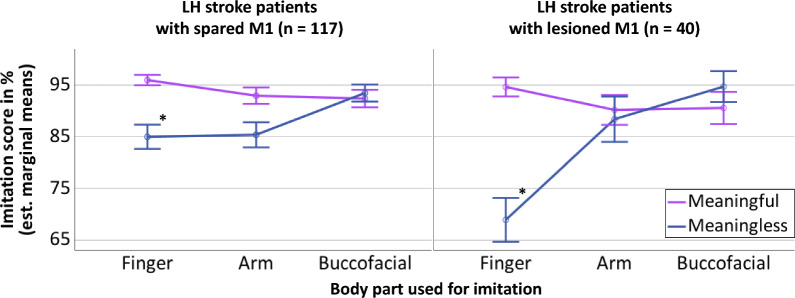
Methods: We identified 157 right-handed patients with first-ever unilateral LH stroke in the sub-acute phase (< 90 days post-stroke), for whom apraxia assessments performed with the ipsilesional left hand and lesion maps were available. Utilizing the maximum probability map of Brodmann area 4 (representing M1) provided by the JuBrain Anatomy Toolbox in SPM, patients were subdivided into two groups depending on whether their lesions involved (n = 40) or spared (n = 117) left M1. We applied a mixed model ANCOVA with repeated measures to compare apraxic deficits between the two patient groups, considering the factors "body part" and "gesture meaning". Furthermore, we explored potential differential effects of the anterior (4a) and posterior (4p) parts of Brodmann area 4 by correlation analyses.
Results: Patients with and without M1 involvement did not differ in age and time post-stroke but in lesion size. When controlling for lesion size, the total apraxia scores did not differ significantly between groups. However, the mixed model ANCOVA showed that LH stroke patients with lesions involving left M1 performed differentially worse when imitating meaningless finger gestures. This effect was primarily driven by lesions affecting Brodmann area 4p.
Conclusions: Even though many current definitions of apraxia disregard a relevant role of (left) M1, the observed differential effect of M1 lesions, specifically involving subarea 4p, on the imitation of meaningless finger gestures in the current sample of LH stroke patients suggests a specific role of left M1 in imitation when high amounts of (motor) attention and sensorimotor integration are required.
Keywords: Body-part specificity; Finger gestures; Gesture meaning; Imitation; Limb-kinetic apraxia; Motor cognition.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The local ethics committee (University of Cologne) approved this single-center, retrospective study, which was carried out under the Declaration of Helsinki. Consent for publication: Not applicable. Competing interests: Gereon R. Fink is a section editor and Peter H. Weiss (-Blankenhorn) is a member of the editorial board of Neurological Research and Practice.
Figures
Similar articles
-
Distinct cognitive components and their neural substrates underlying praxis and language deficits following left hemisphere stroke.Cortex. 2022 Jan;146:200-215. doi: 10.1016/j.cortex.2021.11.004. Epub 2021 Nov 20. Cortex. 2022. PMID: 34896806
-
Gesture meaning modulates the neural correlates of effector-specific imitation deficits in left hemisphere stroke.Neuroimage Clin. 2023;37:103331. doi: 10.1016/j.nicl.2023.103331. Epub 2023 Jan 21. Neuroimage Clin. 2023. PMID: 36716655 Free PMC article.
-
Effect of body-part specificity and meaning in gesture imitation in left hemisphere stroke patients.Neuropsychologia. 2021 Jan 22;151:107720. doi: 10.1016/j.neuropsychologia.2020.107720. Epub 2020 Dec 9. Neuropsychologia. 2021. PMID: 33309676
-
Cerebral correlates of imitation of intransitive gestures: An integrative review of neuroimaging data and brain lesion studies.Neurosci Biobehav Rev. 2018 Dec;95:44-60. doi: 10.1016/j.neubiorev.2018.07.019. Epub 2018 Aug 4. Neurosci Biobehav Rev. 2018. PMID: 30086324 Review.
-
Limb Apraxias: The Influence of Higher Order Perceptual and Semantic Deficits in Motor Recovery After Stroke.Stroke. 2023 Jan;54(1):30-43. doi: 10.1161/STROKEAHA.122.037948. Epub 2022 Dec 21. Stroke. 2023. PMID: 36542070 Review.
References
-
- Rothi, L. J. G., & Heilman, K. M. (1997). Apraxia: The NEUROPSYCHOLOGY OF ACTION. Psychology Press. 10.4324/9781315804545
-
- Schmidt, C. C., & Weiss, P. H. (2022). The cognitive neuroscience of apraxia. In S. Della Sala (Ed.), Encyclopedia of behavioral neuroscience (Vol. 2, pp. 668–677). London: Elsevier. 10.1016/b978-0-12-819641-0.00143-2
-
- Liepmann, H. (1913). Motorische Aphasie und Apraxie. Monatsschrift für Psychiatrie und Neurologie,34, 485–494. 10.1159/000203164
-
- Goldenberg, G. (2014). Apraxia—The cognitive side of motor control. Cortex,57, 270–274. 10.1016/j.cortex.2013.07.016 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources