

Antihypertensive strategies for the prevention of secondary stroke: a systematic review and meta-analysis
- PMID: 39780283
- PMCID: PMC11715515
- DOI: 10.1186/s40001-024-02226-3
Antihypertensive strategies for the prevention of secondary stroke: a systematic review and meta-analysis
Abstract
Background: Stroke is an important contributor to disability and death globally. Hypertension is a main risk factor for recurrent stroke in patients with ischemic and hemorrhagic stroke or transient ischemic attack. Higher systolic blood pressure, diastolic blood pressure, pulse pressure and mean arterial pressure at admission are independently associated with the risk of stroke recurrence. Therefore, lowering blood pressure is recommended by guidelines to prevent the recurrence of stroke.
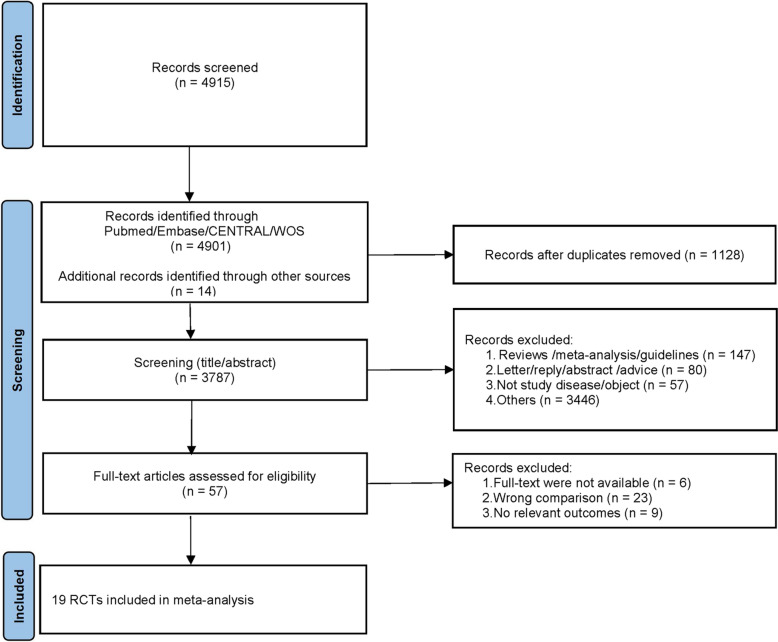
Methods: A systematic search of PubMed, Embase, Cochrane Central Register of Controlled Trials, and Web of Science databases was conducted through January 12, 2024. The search identified randomized controlled trials (RCTs) comparing antihypertensive drugs with control measures (placebo or no treatment) or standard blood pressure control (SBPC) with intensive blood pressure control (IBPC) for recurrent stroke prevention. Primary outcomes included overall and subtype stroke recurrence rates, fatal and non-fatal strokes, cardiovascular deaths, and myocardial infarctions (MIs). Secondary outcomes comprised non-fatal MIs and all-cause mortality. Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated using random or fixed-effect models in Stata 15.0.
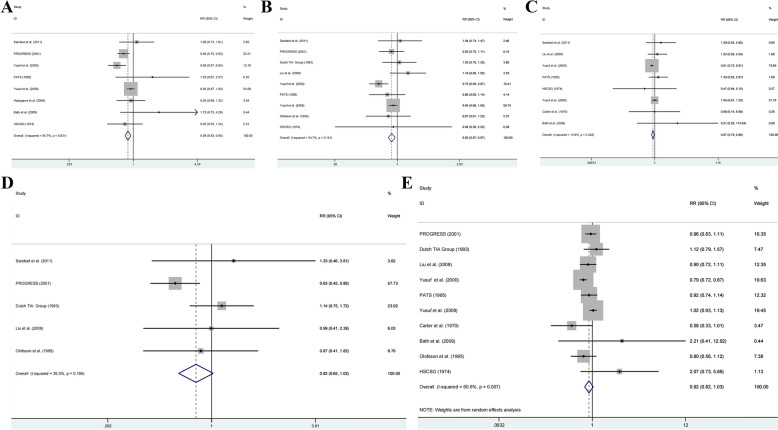
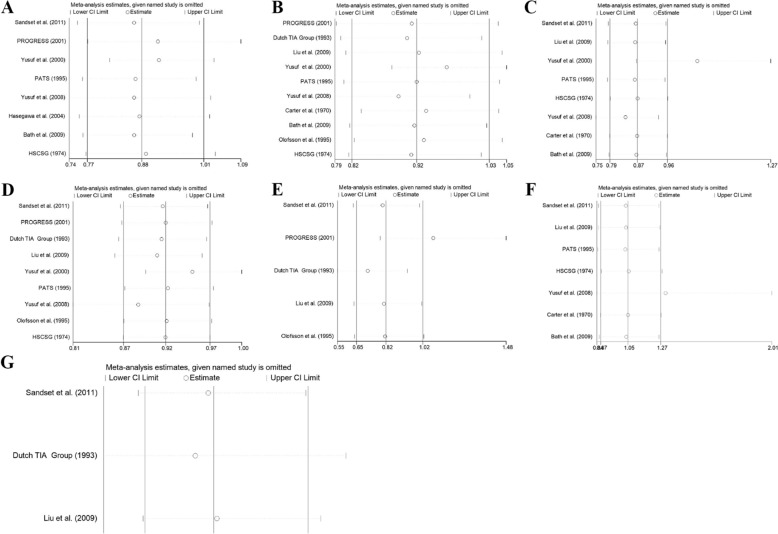
Results: The analysis included 19 RCTs encompassing 72,048 patients. Twelve studies (n = 53,971) evaluated antihypertensive drugs against placebo or no treatment, while seven studies (n = 18,077) compared SBPC with IBPC. Antihypertensive therapy demonstrated significant risk reductions compared to placebo or no treatment for recurrent stroke (RR = 0.86, 95% CI: 0.75-0.97), cardiovascular deaths (RR = 0.92, 95% CI: 0.87-0.97), and MIs (RR = 0.87, 95% CI: 0.79-0.96). IBPC showed superior outcomes compared to SBPC, with significant reductions in recurrent stroke (RR = 0.87, 95% CI: 0.77-0.98), cardiovascular deaths (RR = 0.75, 95% CI: 0.61-0.91), and all-cause mortality (RR = 0.85, 95% CI: 0.73-0.95).
Conclusion: In stroke patients, antihypertensive therapy demonstrates significant protective effects against stroke recurrence, cardiovascular deaths, and MIs compared to placebo or no treatment. Additionally, IBPC provides enhanced protection against stroke recurrence, cardiovascular deaths, and all-cause mortality compared to SBPC.
Keywords: Antihypertensive therapy; Blood pressure management; Hypertension; Meta-analysis; Recurrent stroke; Secondary prevention; Stroke.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures






References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
