

How Accurately Does Bone Mineral Density Predict Bone Strength? A Clinical Observational Study of Osteoporosis Vertebral Compression Fractures in Postmenopausal Women
- PMID: 39780751
- PMCID: PMC11962276
- DOI: 10.1111/os.14354
How Accurately Does Bone Mineral Density Predict Bone Strength? A Clinical Observational Study of Osteoporosis Vertebral Compression Fractures in Postmenopausal Women
Abstract
Objectives: Dual energy x-ray absorptiometry (DXA) provides incomplete information about bone strength. There are few data on the relationship between osteoporosis-related examinations and bone strength. The objective of the present study was to determine which osteoporosis-related examinations best predicted trabecular bone strength, and to enhance a formula for predicting bone strength on the basis of bone density examination.
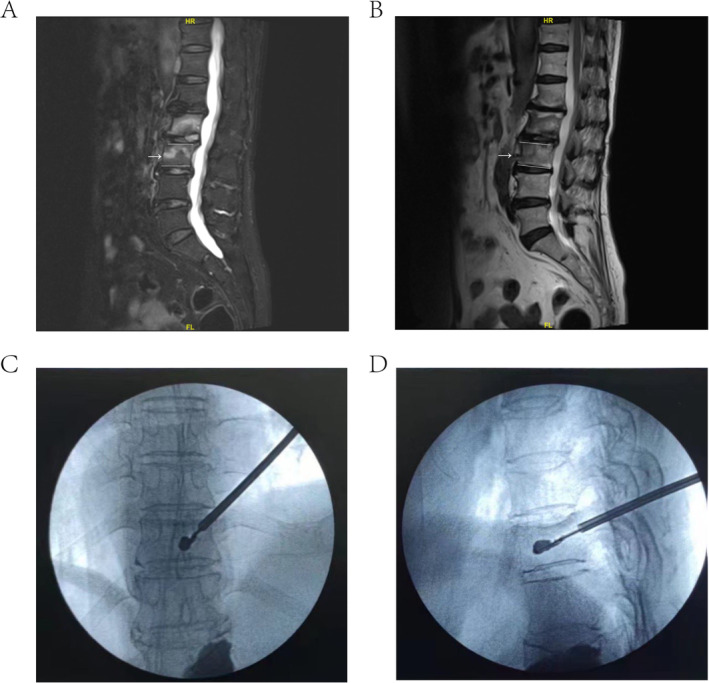
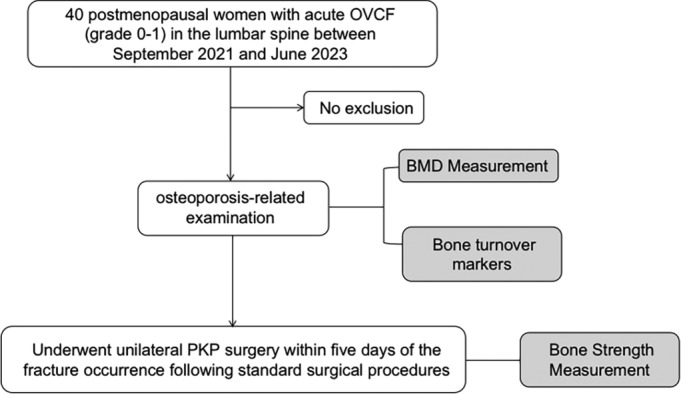
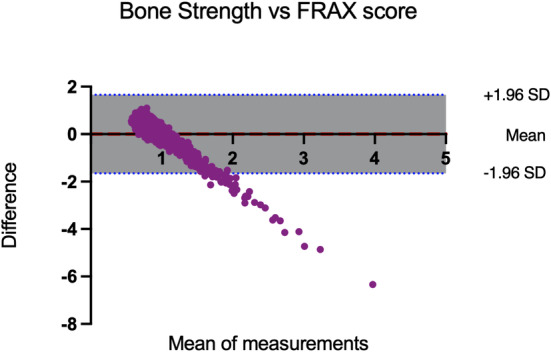
Methods: This observational study included postmenopausal women (aged over 50 years) who underwent unilateral percutaneous kyphoplasty (PKP) surgery in the lumbar spine between September 2021 and June 2023. The pressure within each balloon expansion circle was extracted to reflect the true bone strength. The NHANES 2013-2014 data were used to assess the performance of the formula. The performance of the formula was compared with that of the observed actual fractures. Bland-Altman analysis was used to compare the agreement between the formula and the fracture risk assessment tool (FRAX) score.
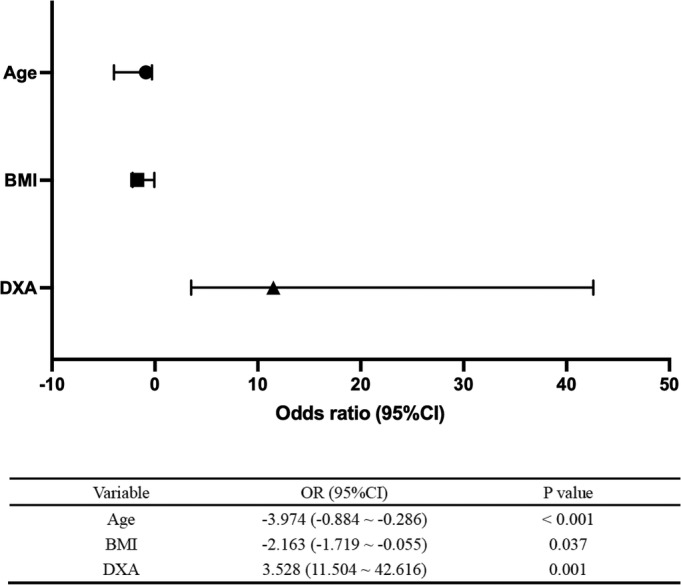
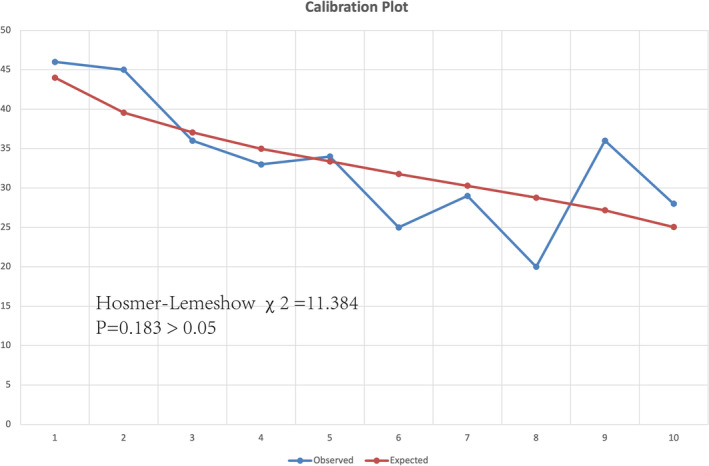
Results: A total of 40 postmenopausal women (mean age ± standard deviation, 70.90 years ± 10.30) were enrolled. The average balloon pressure was 59.23 psi (± 12.40, means ± SDs). The mean BMD of total lumbar spine (average of L1-L4) was 0.89 g/cm2 ± 0.20 (mean ± standard), and the Pearson correlation coefficient between lumbar BMD and bone strength was 0.516. After adjusting for age and BMI, the DXA response rate to bone strength reached 72%. Calibration plots of the observed actual fractures versus those estimated via the bone strength formula were considered good fits. The Bland-Altman analysis revealed a nonsignificant difference between the formula and the FRAX score in predicting fracture risk.
Conclusions: After adjustment, the DXA response rate to bone strength reached 72%, indicating a strong correlation. In addition, Bone Strength = DXA × 27 - Age × 0.585-BMI × 0.887 + 98.
Keywords: balloon pressure; bone mineral density (BMD); bone strength; dual energy x‐ray absorptiometry (DXA); percutaneous kyphoplasty (PKP)surgery.
© 2025 The Author(s). Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Blake G. M. and Fogelman I., “The Clinical Role of Dual Energy X‐Ray Absorptiometry,” European Journal of Radiology 71, no. 3 (2009): 406–414. - PubMed
-
- Cummings S. R., Bates D., and Black D. M., “Clinical Use of Bone Densitometry: Scientific Review,” Journal of the American Medical Association 288, no. 15 (2002): 1889–1897. - PubMed
-
- Khan A. A., Slart R., Ali D. S., et al., “Osteoporotic Fractures: Diagnosis, Evaluation, and Significance From the International Working Group on DXA Best Practices,” Mayo Clinic Proceedings 99, no. 7 (2024): 1127–1141. - PubMed
-
- de Bakker C. M. J., Tseng W. J., Li Y., Zhao H., and Liu X. S., “Clinical Evaluation of Bone Strength and Fracture Risk,” Current Osteoporosis Reports 15, no. 1 (2017): 32–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
