

Social network analysis as a new tool to measure academic impact of physicians
- PMID: 39780864
- PMCID: PMC11705531
- DOI: 10.1002/lio2.70060
Social network analysis as a new tool to measure academic impact of physicians
Abstract
Introduction: H-index is a widely used metric quantifying a researcher's productivity and impact based on an author's publications and citations. Though convenient to calculate, h-index fails to incorporate collaborations and interrelationships between physicians into its assessment of academic impact, leading to limited insight into grouped networks. We present social network analysis as a tool to measure relationships between physicians and quantify their academic impact.
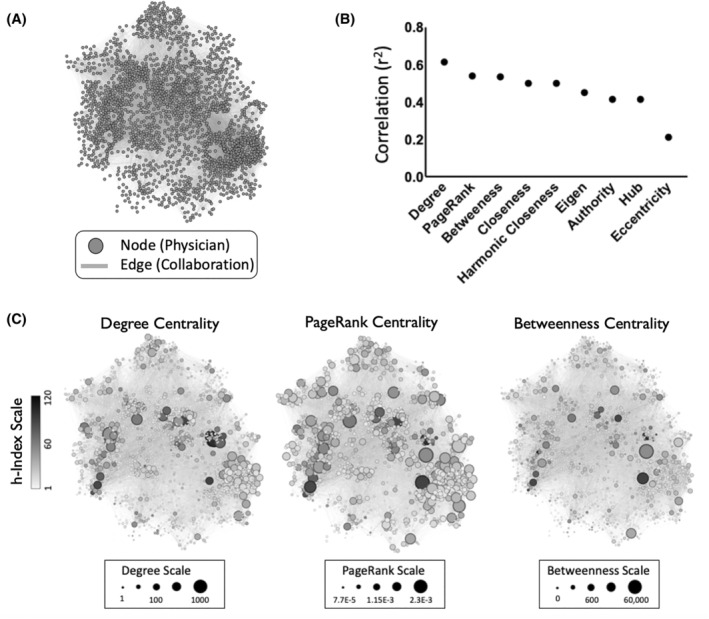
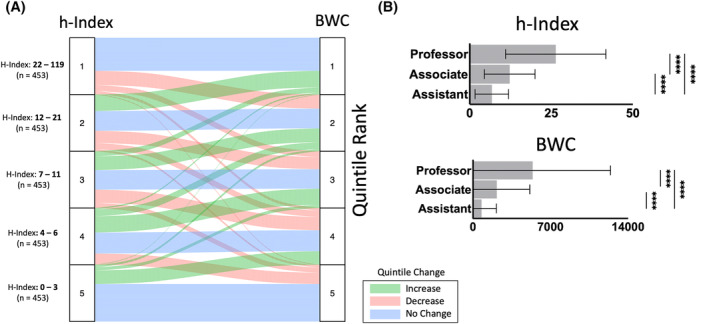
Methods: A bibliometric multicenter analysis was conducted on physician faculty from 129 US ACGME accredited otolaryngology programs who have publications with a physician co-author in the field. Using web searches, 2494 physician faculty were identified. Scopus IDs, h-indices, and publication data for these physicians were identified using multiple Elsevier APIs queried in December 2023. Publications with multiple otolaryngology physician co-authors were included. Network and sub network maps were generated using Gephi and analyzed with custom R scripts. Centrality measures (degree, PageRank, betweenness centralities) quantified collaboration propensity. Non-parametric correlation analysis between centrality measures and h-index was conducted. Sankey diagrams were plotted using ggplot2.
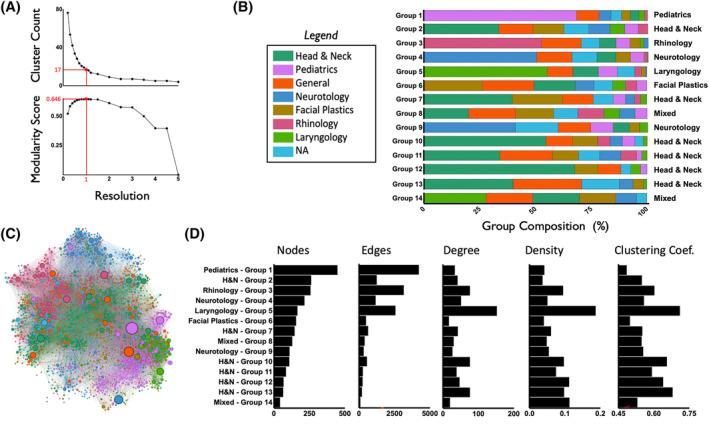
Results: A co-authorship network of 2259 physicians was constructed. Physicians were visualized as nodes with collaborations as links. Centrality measures correlated strongly with h-index (h-index vs. degree centrality: r 2 = 0.62, h-index vs. PageRank: r 2 = 0.55, h-index vs. betweenness centrality: r 2 = 0.55; p < .0001). Analysis revealed novel insights into physician network structure, identifying 14 communities primarily populated by single subspecialties with varied node density.
Conclusion: Social network analysis showed moderate correlation between social connectedness measures and h-index, supporting its use in measuring academic impact. In otolaryngology, collaborative interactions within the academic community are strongly shaped by sub-specialty affiliation and academic institution.
Keywords: academic otolaryngology; faculty; h‐index; otolaryngology; publication; social network.
© 2025 The Author(s). Laryngoscope Investigative Otolaryngology published by Wiley Periodicals LLC on behalf of The Triological Society.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Network effects on scientific collaborations.PLoS One. 2013;8(2):e57546. doi: 10.1371/journal.pone.0057546. Epub 2013 Feb 28. PLoS One. 2013. PMID: 23469021 Free PMC article.
-
Academic Productivity of US Neurosurgery Residents as Measured by H-Index: Program Ranking with Correlation to Faculty Productivity.Neurosurgery. 2017 Jun 1;80(6):975-984. doi: 10.1093/neuros/nyx071. Neurosurgery. 2017. PMID: 28368531
-
c-index and Subindices of the h-index: New Variants of the h-index to Account for Variations in Author Contribution.Cureus. 2018 May 15;10(5):e2629. doi: 10.7759/cureus.2629. Cureus. 2018. PMID: 30027021 Free PMC article.
-
Academic productivity and contributions to the literature among spine surgery fellowship faculty.Spine J. 2015 Oct 1;15(10):2126-31. doi: 10.1016/j.spinee.2015.03.026. Epub 2015 Mar 21. Spine J. 2015. PMID: 25804116 Review.
-
A social network analysis of an epistemic community studying neoliberal conservation.Conserv Biol. 2025 Apr;39(2):e70001. doi: 10.1111/cobi.70001. Conserv Biol. 2025. PMID: 40165691 Free PMC article. Review.
References
{kind=link}
LinkOut - more resources
Full Text Sources