

doi: 10.1016/j.eats.2024.103221.
eCollection 2024 Dec.
Basic Hip Arthroscopy Part 2: Central Compartment Arthroscopy (Interportal Capsulotomy, Acetabuloplasty, and Labral Repair)
Affiliations
- PMID: 39780879
- PMCID: PMC11704905
- DOI: 10.1016/j.eats.2024.103221
Item in Clipboard
Basic Hip Arthroscopy Part 2: Central Compartment Arthroscopy (Interportal Capsulotomy, Acetabuloplasty, and Labral Repair)
Arthrosc Tech.
.
Abstract
Over the past decade, hip-preservation strategies have gained momentum, resulting in a notable increase in the use of hip arthroscopy for diagnostic and therapeutic interventions in hip-related pathology. In this 3-part series, the authors will aim to comprehensively review the fundamentals of hip arthroscopy in the setting of femoroacetabular impingement. This Technical Note will thoroughly review the senior authors' approach to managing the central compartment of the hip in the context of femoroacetabular impingement.
© 2024 The Authors.
Figures
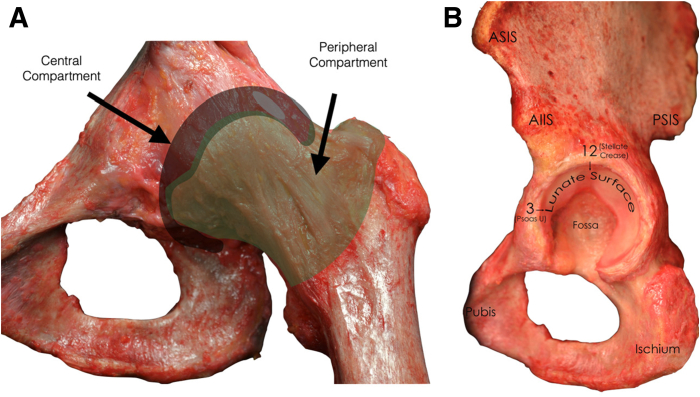
(A) Cadaveric dissection of a left hip with highlighted appreciation of the arthroscopic central and peripheral compartments as viewed from the anterior/coronal plane. (B) Sagittal view of cadaveric dissection demonstrating the hip’s central compartment, including the labrum, articular lunate surface, and cotyloid fossa. Demonstration of where it lies in relation to the anterior superior iliac spine (ASIS), anterior inferior iliac spine (AIIS), posterior superior iliac spine (PSIS), pubis, and ischium is also represented.
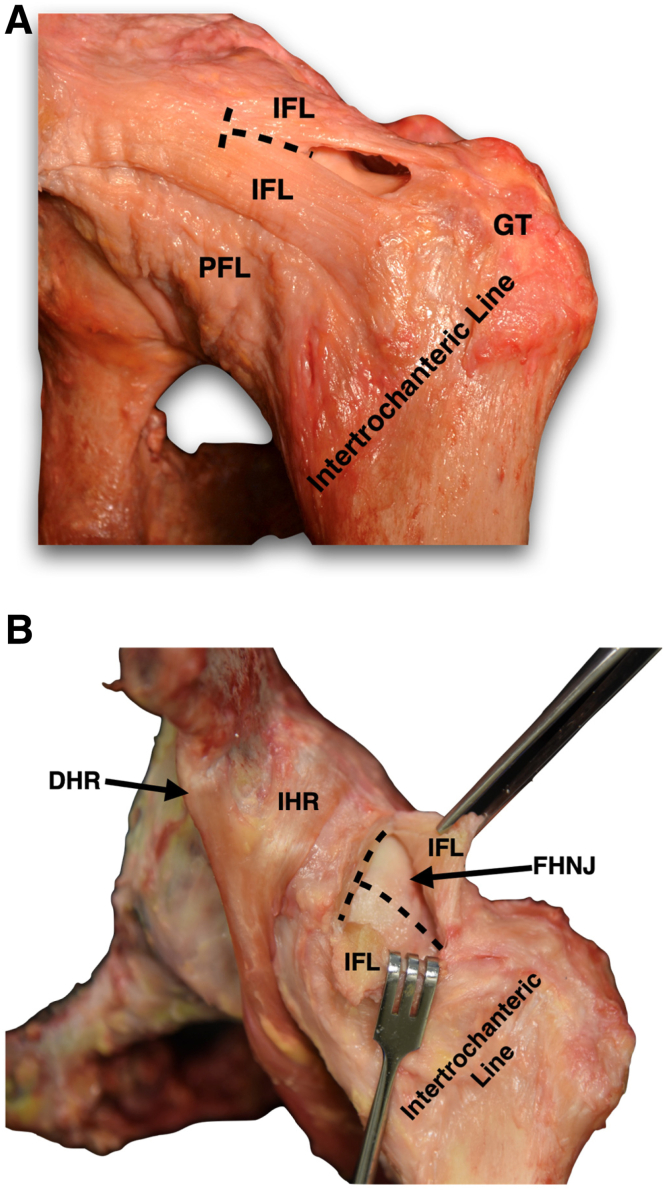
(A) Cadaveric dissection of a left hip’s anterior capsule. The iliofemoral ligament (IFL) is incised for the creation of the interportal and subsequent T capsulotomies (dotted lines), allowing for exposure of the central and peripheral compartments, respectively. Also seen are the pubofemoral ligament (PFL), greater trochanter (GT), and the intertrochanteric line. (B) Cadaveric representation of the interportal and T capsulotomies. Medial and lateral IFL leaflets are created upon completion of the T capsulotomy exposing the femoral head-neck junction (FHNJ). The direct and indirect heads of the rectus femoris are also appreciated on the image (DHR and IHR, respectively).
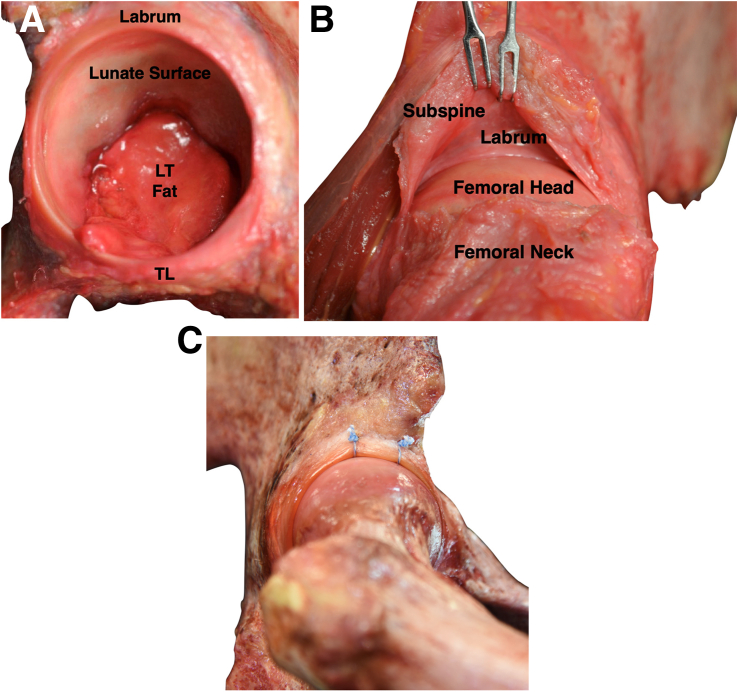
(A) Sagittal view of a left hip cadaveric dissection demonstrating the labrum surrounding the acetabular edge as well as the C-shaped articular cartilage (lunate surface) with the ligamentum teres (LT) fat in the center of the acetabular notch. Interruption of the labrum and articular cartilage can be observed inferiorly at the level of the transverse ligament (TL). (B) Appreciation of the subspinal space demonstrated in a cadaveric model of a left hip. (C) Cadaveric dissection of a right hip after performance of a labral repair.
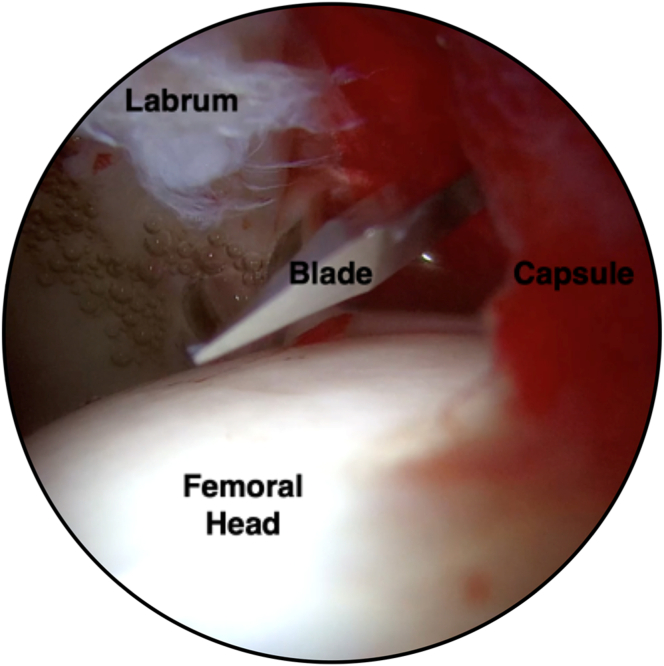
Arthroscopic image of the right hip demonstrating blade insertion through the modified midanterior portal for creation of the interportal capsulotomy as viewed from the anterolateral portal.
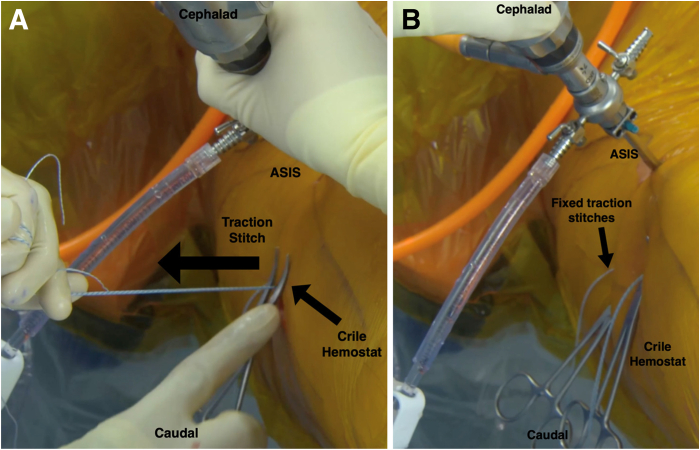
(A) Surgical-site image of capsular traction stitches being fixed over the skin in a right hip arthroscopy. The traction stitches are placed through capsular tissue and manually tensioned to allow for retraction of the capsular tissue outside the arthroscopic viewpoint. A Crile hemostat is placed atop the skin while holding traction of the previously placed stitches. (B) Tension is kept by locking the suture within the Crile hemostat just proud with the patient’s skin in aims of avoiding macerating the patient’s skin.
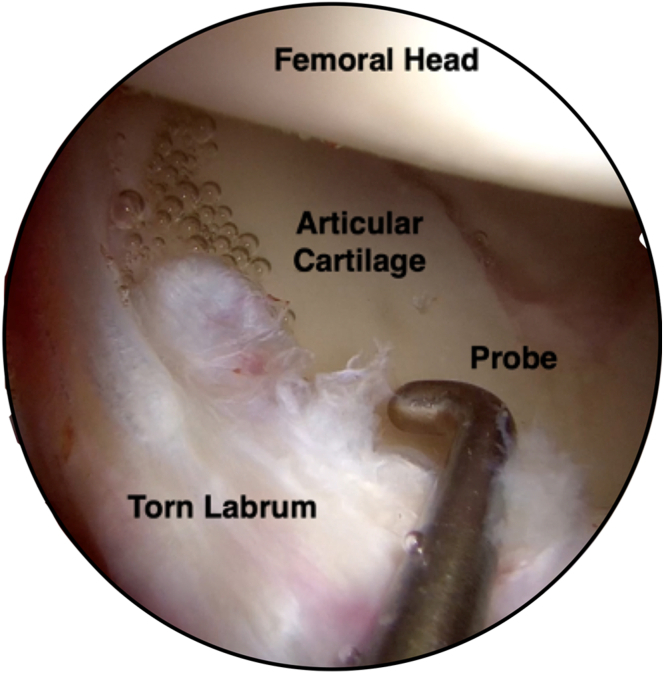
Arthroscopic image of the right hip demonstrating a torn labrum extending from the 12-to 2-o’clock position as viewed from the modified midanterior portal. A probe is being used for assessment of labral stability given the associated tear.
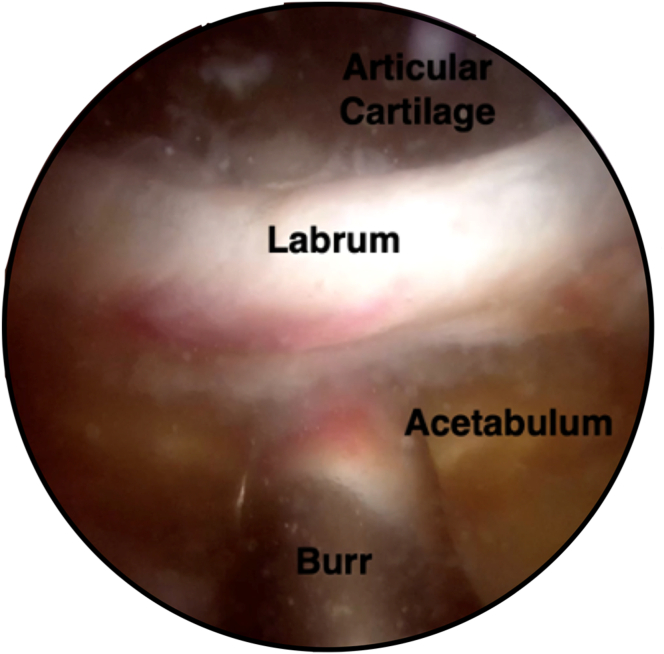
Right hip arthroscopic image demonstrating a burr performing the acetabular rim trimming in preparation for anchor deployment as viewed from the modified midanterior portal.
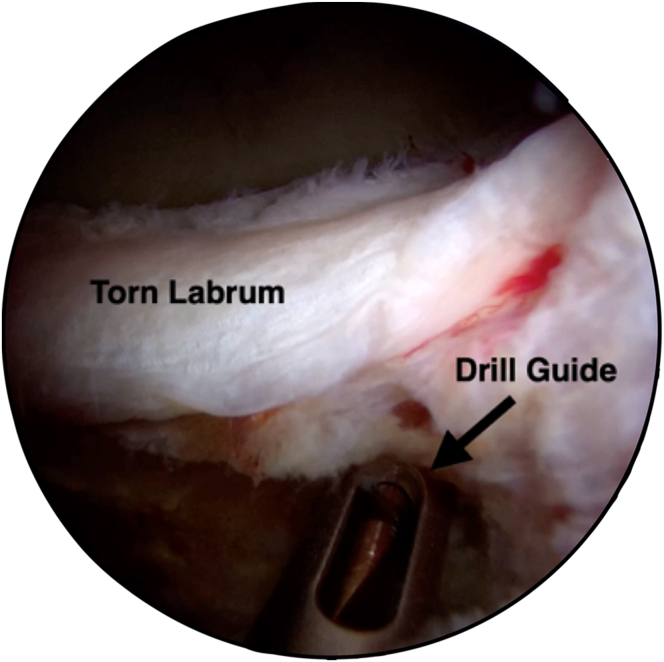
Arthroscopic image of the right hip demonstrating drilling of the acetabulum for subsequent anchor deployment at the 12-o’clock position as viewed from the modified midanterior portal. Fraying of the labrum and medial chondrolabral junction disruption can also be appreciated.
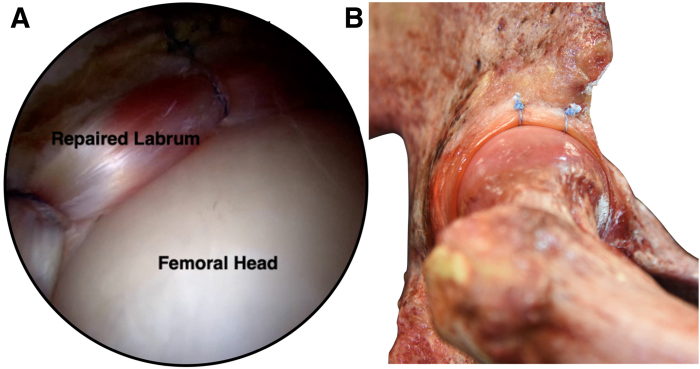
(A) Arthroscopic image showing completion of the right labral repair with restoration of the hip’s native suction seal as viewed from the modified midanterior portal. (B) Cadaveric demonstration of labral repair with achievement of the hip’s native suction seal as viewed from a sagittal view.
Similar articles
-
Basic Hip Arthroscopy Part 3: Peripheral-Compartment Arthroscopy (T-Capsulotomy, Femoroplasty, and Capsular Closure).Arthrosc Tech. 2024 Sep 7;13(12):103222. doi: 10.1016/j.eats.2024.103222. eCollection 2024 Dec. Arthrosc Tech. 2024. PMID: 39780874 Free PMC article.
-
Basic Hip Arthroscopy Part 1: Patient Positioning and Portal Placement.Arthrosc Tech. 2024 Aug 31;13(12):103220. doi: 10.1016/j.eats.2024.103220. eCollection 2024 Dec. Arthrosc Tech. 2024. PMID: 39780875 Free PMC article.
-
Achievement of Meaningful Clinical Outcomes Is Unaffected by Capsulotomy Type During Arthroscopic Treatment of Femoroacetabular Impingement Syndrome: Results From the Multicenter Arthroscopic Study of the Hip (MASH) Study Group.Am J Sports Med. 2021 Mar;49(3):713-720. doi: 10.1177/0363546520987226. Epub 2021 Feb 9. Am J Sports Med. 2021. PMID: 33560868
-
The Role of Comprehensive Capsular Management in Hip Arthroscopy for the Treatment of Femoroacetabular Impingement Syndrome.Arthroscopy. 2020 Jan;36(1):9-11. doi: 10.1016/j.arthro.2019.10.028. Arthroscopy. 2020. PMID: 31864606 Review.
-
Systematic Review of Hip Arthroscopy for Femoroacetabular Impingement: The Importance of Labral Repair and Capsular Closure.Arthroscopy. 2019 Feb;35(2):646-656.e3. doi: 10.1016/j.arthro.2018.09.005. Arthroscopy. 2019. PMID: 30712639
Cited by
-
Hip Arthroscopic Labral Repair With Transcapsular Suture Passage for Medial Capsular Preservation.Arthrosc Tech. 2025 May 22;14(7):103647. doi: 10.1016/j.eats.2025.103647. eCollection 2025 Jul. Arthrosc Tech. 2025. PMID: 40822177 Free PMC article.
References
-
- Lynch T.S., Bedi A., Larson C.M. Athletic hip injuries. J Am Acad Orthop Surg. 2017;25:269–279. - PubMed
-
- Goto T., Hamada D., Mineta K., et al. The state of the art in arthroscopic hip surgery. J Med Invest. 2014;61:226–232. - PubMed
-
- Duchman K.R., Westermann R.W., Glass N.A., Bedard N.A., Mather R.C., Amendola A. Who is performing hip arthroscopy? An analysis of the American Board of Orthopaedic Surgery Part-II Database. J Bone Joint Surg Am. 2017;99:2103–2109. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
