

Long Head of Biceps Tenodesis for Maintaining Inherent Length and Uniform Tension at the Bicipital Groove: Suprapectoral Double-Row Technique With All-Suture Anchors
- PMID: 39780901
- PMCID: PMC11704907
- DOI: 10.1016/j.eats.2024.103130
Long Head of Biceps Tenodesis for Maintaining Inherent Length and Uniform Tension at the Bicipital Groove: Suprapectoral Double-Row Technique With All-Suture Anchors
Abstract
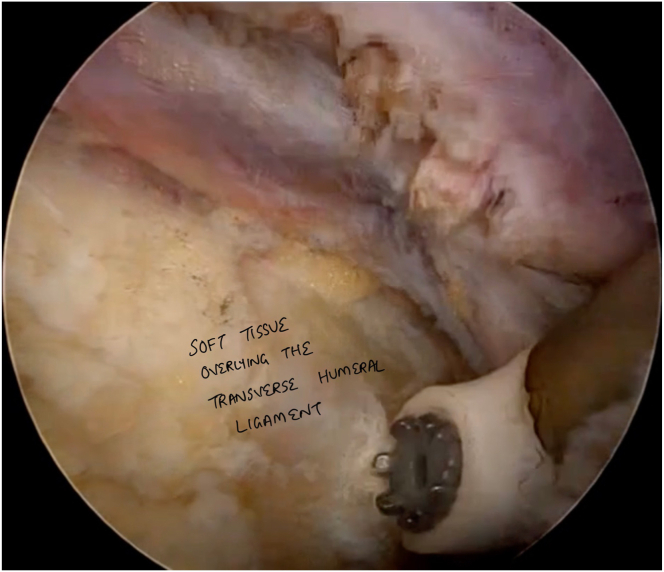
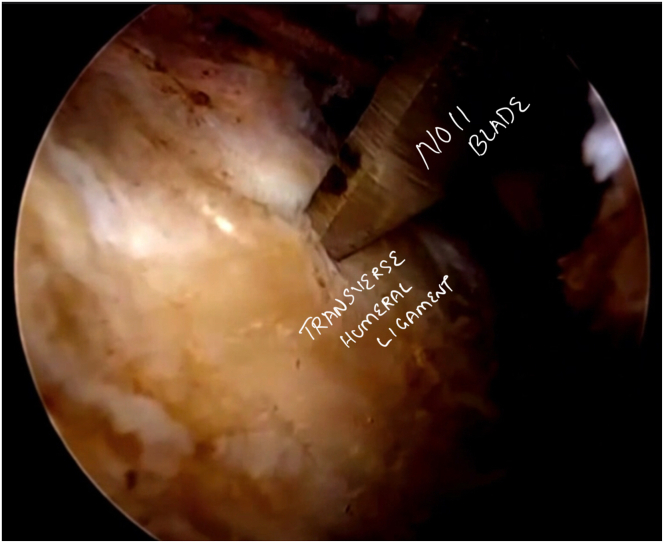
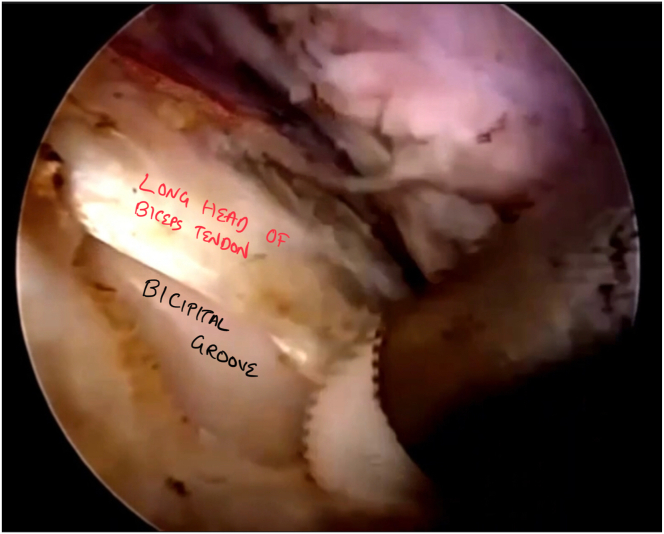
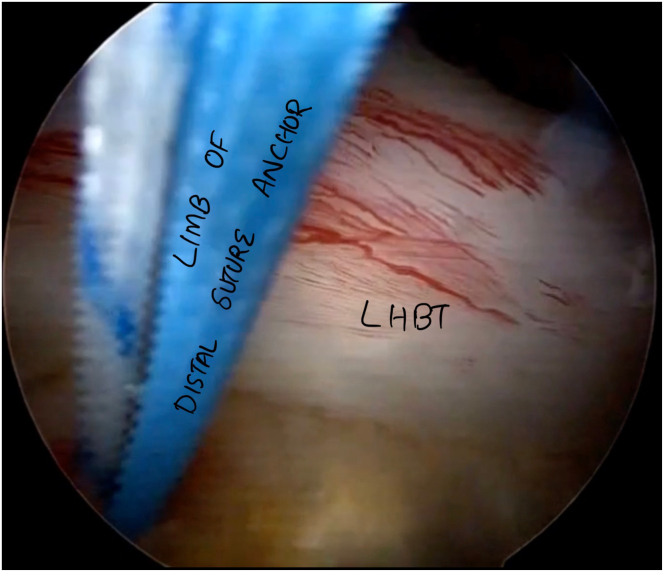
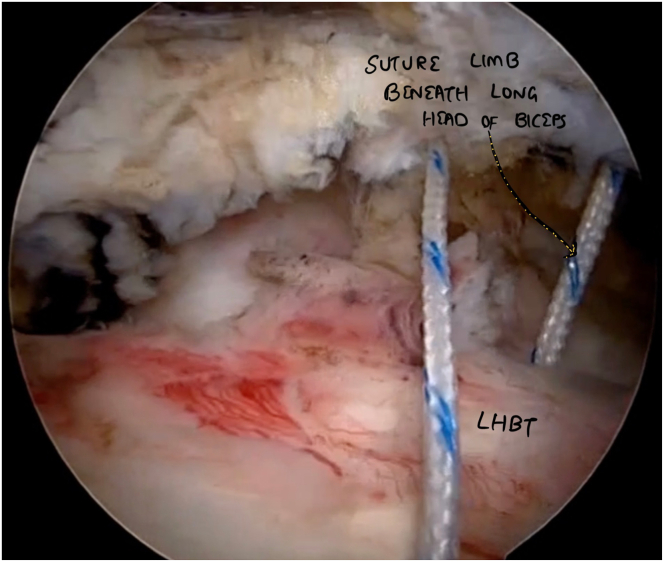
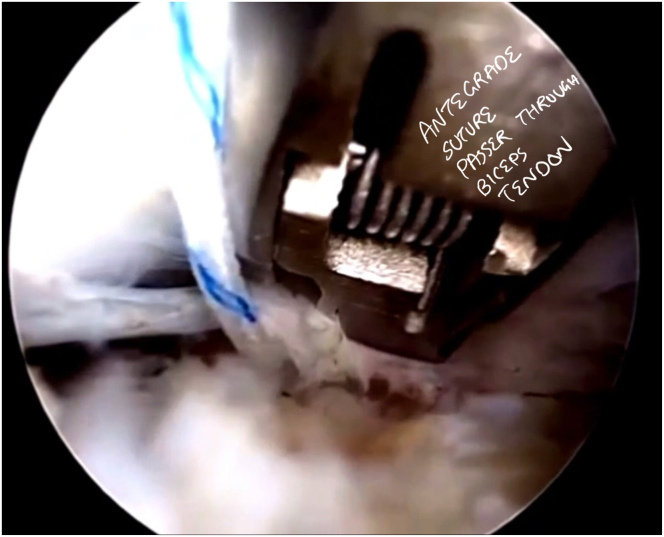
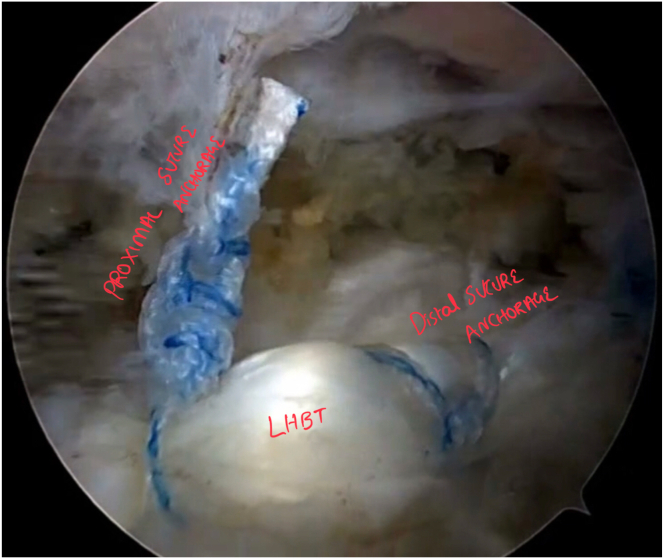
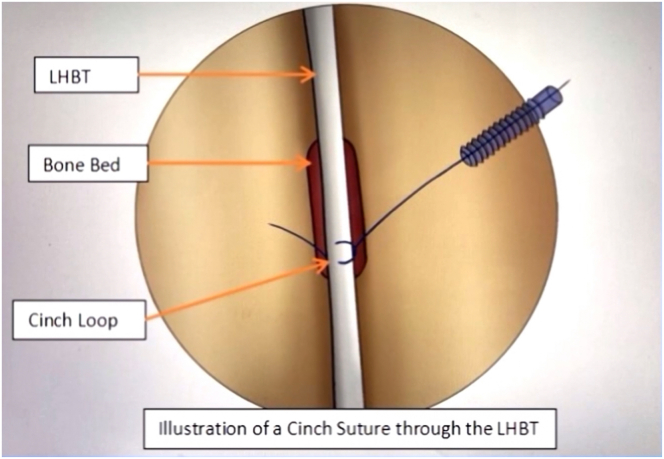
The clinicopathologic conditions of the long head of the biceps tendon vary, encompassing tendinitis, peritendinous inflammation, hypertrophy, and partial or complete tears. These symptoms are typically linked with SLAP tears and instability of the long head of the biceps tendon, often resulting in partial displacement or complete dislocation. The choice between tenotomy and tenodesis depends on varied factors. The choice of suprapectoral or subpectoral tenodesis is a difficult decision and should be weighed on a tailored basis. Our approach to suprapectoral tenodesis presents a blend of factors, maintaining uniform tension in the bicipital groove, limiting the number of portals for arthroscopy, re-tensioning the tendon after initial anchor placement, and preserving the inherent length of the functional biceps tendon without compromising its quality.
© 2024 The Authors.
Figures
References
LinkOut - more resources
Full Text Sources
