

Development and validation of clinical criteria for critical illness-associated immune dysfunction: based on the MIMIC-IV database
- PMID: 39780936
- PMCID: PMC11707548
- DOI: 10.3389/fmed.2024.1465397
Development and validation of clinical criteria for critical illness-associated immune dysfunction: based on the MIMIC-IV database
Abstract
Background: Critical illness-associated immune dysfunction (CIID) is prevalent in the ICU and frequently resulted in uncontrollably immune responses. Critical immunological dysfunction is understood to be important, although there are currently no clinically accepted diagnostic criteria for it. Given this, we examined the literature and developed an initial diagnostic criterion that we validated using the MIMIC-IV database.
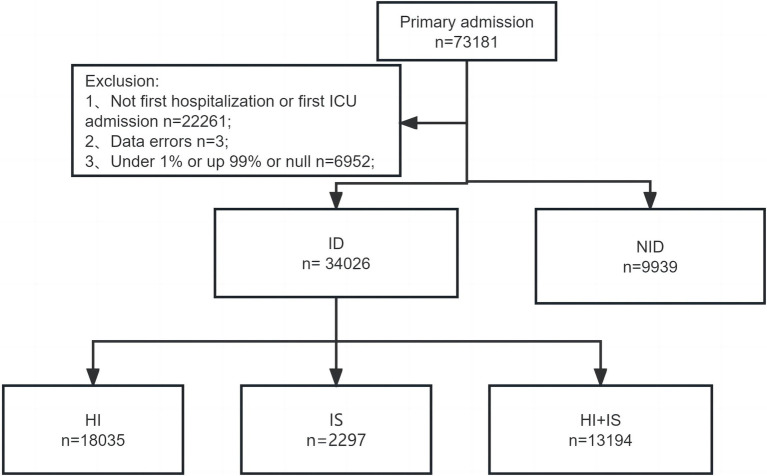
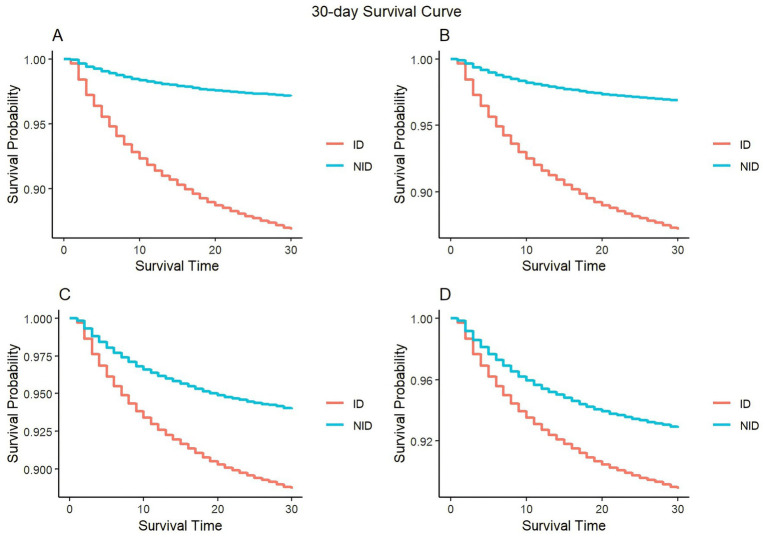
Methods: We searched the related literature in the last 32 years. Patients admitted to the ICU for the first time were selected by screening the MIMIC-IV database. Different criteria were used to categorize patients into groups related to immune dysfunction (ID) and non-immune dysfunction (NID). Within the ID group, patients were subdivided into three subgroups: hyperinflammatory (HI), immunosuppression (IS), and a subgroup combining immunosuppression and hyperinflammation (HI+IS). The APACHE II was used to measure the patients' severity. The association between immune dysfunction and mortality after 30 or 180 days was evaluated through the KM curves and COX regression analysis.
Results: By summarizing relevant literature, we proposed the initial diagnostic criteria. The analysis included 43,965 patients, with approximately 77% meeting the diagnostic criteria for CIID. We observed that patients with immune dysfunction possessed higher APACHE II scores and there were differences in peak APACHE II among the three subgroups. When comparing patients' 30-day mortality in the COX model, it is evident that patients in the IS subgroup had the lowest risk and patients in the HI subgroup the greatest risk after accounting for all covariates. In contrast, patients in the IS subgroup had the highest risk of death, those in the HI subgroup had the lowest risk when comparing long-term mortality. In summary, we propose and validate diagnostic criteria related to CIID. Subgroup analyses were carried out, which also revealed variations between the three groups.
Conclusion: The diagnostic criteria were confirmed by the MIMIC-IV database, demonstrating the diagnostic criteria were scientifically valid and reliable.
Keywords: MIMIC-IV; critical immunological dysfunction; hyperinflammatory; immune responses; immunosuppression.
Copyright © 2024 Zhou, Tao, Yang, Li and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources