

Pipeline esophageal varices: Insights from clinical cases and models
- PMID: 39781208
- PMCID: PMC11706798
- DOI: 10.1002/deo2.70054
Pipeline esophageal varices: Insights from clinical cases and models
Abstract
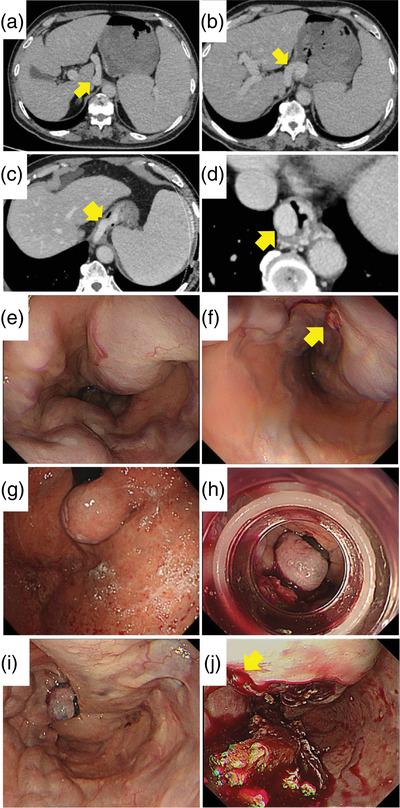
Objectives: While esophageal varices (EVs) are typically treated endoscopically, other options such as interventional radiology or surgical treatment are considered when endoscopic treatment is challenging. Pipeline EVs are difficult to treat endoscopically due to their large diameter, and currently, no specific treatment guidelines have been established.
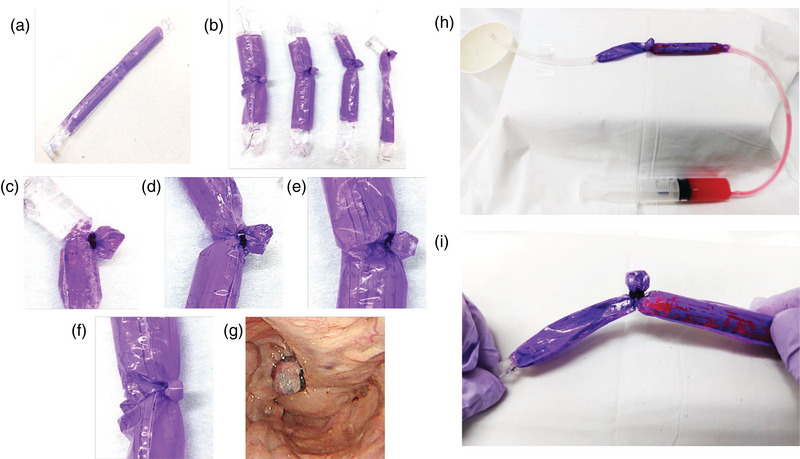
Methods: We reviewed cases of pipeline EVs treated at our hospital and analyzed previously reported cases to collect evidence for the formulation of treatment guidelines. Additionally, we created EV simple models to evaluate the safety margin of endoscopic variceal ligation for varices.
Results: Our analysis included 14 cases of pipeline EVs (four cases treated at our hospital from 2013 to 2024 and 10 previously reported cases from 1990 to 2024). Endoscopic treatment alone was insufficient in six cases (42.9%), and five cases (35.7%) required interventional radiology or surgical intervention. Using EV simple models with varying diameters, EVL was inadequate for varices with diameters of 20 mm or larger.
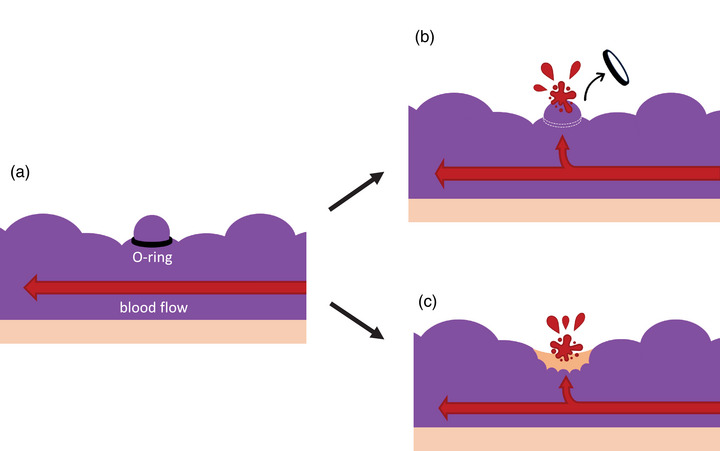
Conclusions: There are few reported cases of pipeline EVs, making it difficult to determine a treatment algorithm. In our study using an EV simple model, it was suggested that endoscopic variceal ligation is effective in blocking blood flow for EVs with a diameter of 15 mm or less. It is important that we understand there are EVs, such as pipeline EVs, for which there are limitations to safely occluding blood flow with endoscopic variceal ligation, and it may be necessary to develop treatment strategies that include methods other than endoscopic therapy.
Keywords: endoscopic injection sclerotherapy; endoscopic variceal ligation; esophageal varices; giant esophageal varices; pipeline esophageal varices.
© 2025 The Author(s). DEN Open published by John Wiley & Sons Australia, Ltd on behalf of Japan Gastroenterological Endoscopy Society.
Conflict of interest statement
None.
Figures
Similar articles
-
Evaluation and management of esophageal varices by through-the-scope endoscopic Doppler probe method.Dig Endosc. 2022 Nov;34(7):1370-1379. doi: 10.1111/den.14345. Epub 2022 Jun 12. Dig Endosc. 2022. PMID: 35488450
-
Ligation plus low-volume sclerotherapy for high-risk esophageal varices: comparisons with ligation therapy or sclerotherapy alone.J Gastroenterol. 1998 Feb;33(1):1-5. doi: 10.1080/00365529850166112. J Gastroenterol. 1998. PMID: 9497213 Clinical Trial.
-
Novel balloon compression-assisted endoscopic injection sclerotherapy and endoscopic variceal ligation in the treatment of esophageal varices: a prospective randomized study.Surg Endosc. 2022 Oct;36(10):7839-7847. doi: 10.1007/s00464-022-09412-6. Epub 2022 Jul 25. Surg Endosc. 2022. PMID: 35879573 Free PMC article. Clinical Trial.
-
Treatment modalities for bleeding esophagogastric varices.J Nippon Med Sch. 2012;79(1):19-30. doi: 10.1272/jnms.79.19. J Nippon Med Sch. 2012. PMID: 22398787 Review.
-
Low risk of bacteremia after endoscopic variceal therapy for esophageal varices: a systematic review and meta-analysis.Endosc Int Open. 2015 Oct;3(5):E409-17. doi: 10.1055/s-0034-1392552. Epub 2015 Aug 11. Endosc Int Open. 2015. PMID: 26528494 Free PMC article. Review.
Cited by
-
Management Strategies for Refractory Esophageal Varices.DEN Open. 2025 Jun 19;6(1):e70155. doi: 10.1002/deo2.70155. eCollection 2026 Apr. DEN Open. 2025. PMID: 40538992 Free PMC article. Review.
References
-
- Obara K, Hikichi T, Shibukawa G et al. Endoscopic injection sclerotherapy for pipeline varix. Gastroenterol Endosc 2009; 21: 847–854. (in Japanese).
-
- Toyonaga A, Iwao T, Sumino M et al. Distinctive portal venographic pattern in patients with sclerotherapy resistant oesophageal varices. J Gastroenterol Hepatol 1996; 11: 1110–1114. - PubMed
-
- Hashizume M, Tanoue K, Kitano S, Ohta M, Sugimachi K. Giant bar‐type esophageal varices not eradicated by repeated injection sclerotherapy. Gastrointest Endosc 1991; 37: 187–189. - PubMed
-
- Hamaguchi M, Higuchi K, Ando K et al. Efficacy of combination of endoscopic variceal ligation with sclerotherapy on pipe‐line varix: Report of a case. Gastroenterol Endosc 1999; 41: 65–71. (in Japanese).
-
- Chikamori F. Endoscopic injection sclerotherapy with simultaneous ligation (EISL) for the treatment of esophagogastric varices. Gastroenterol Endosc 2017; 59: 1337–1343. (in Japanese).
LinkOut - more resources
Full Text Sources