

Quantifying the potential contribution of drugs to the occurrence of acute kidney injury in patients with chronic kidney disease
- PMID: 39781474
- PMCID: PMC11707387
- DOI: 10.1093/ckj/sfae357
Quantifying the potential contribution of drugs to the occurrence of acute kidney injury in patients with chronic kidney disease
Abstract
Background: We sought to comprehensively describe drug-related components associated with acute kidney injury (AKI) in patients with chronic kidney disease (CKD), describing the incidence of drug-related AKI, the proportion of preventable AKI, identified the various drugs potentially associated with it, explored the risk factors, and assessed the 1-year incidences of the recurrence of drug-related AKI, kidney failure, and death.
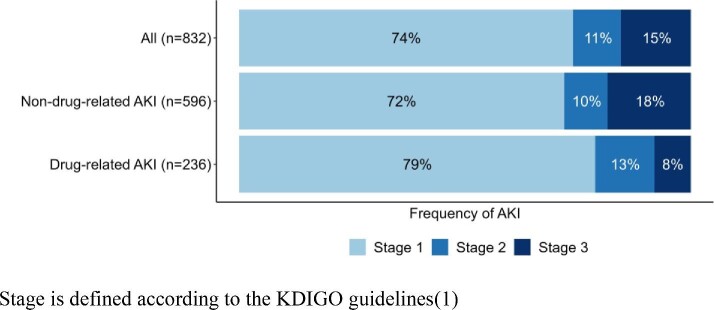
Methods: CKD-REIN is a French national prospective cohort of 3033 nephrology outpatients with a confirmed diagnosis of CKD (eGFR <60 ml/min/1.73 m²). AKIs and adverse drug reactions (ADRs) were prospectively identified from hospital reports, medical records, and patient interviews. Expert nephrologists used the KDIGO criteria to adjudicate all stages of AKI, and expert pharmacologists used validated tools to adjudicate ADRs (including drug-related AKIs).
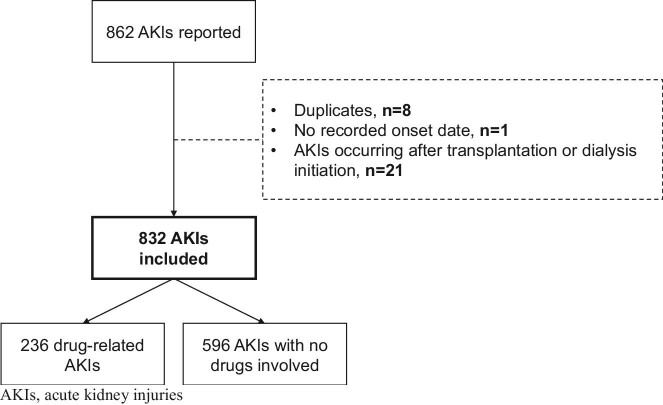
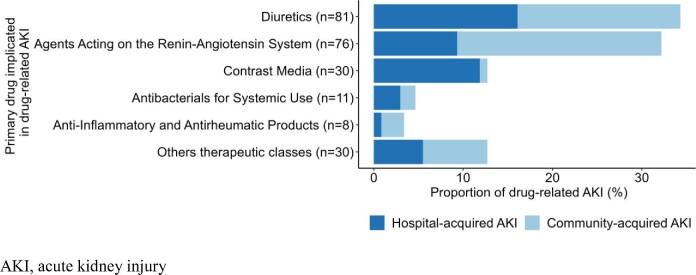
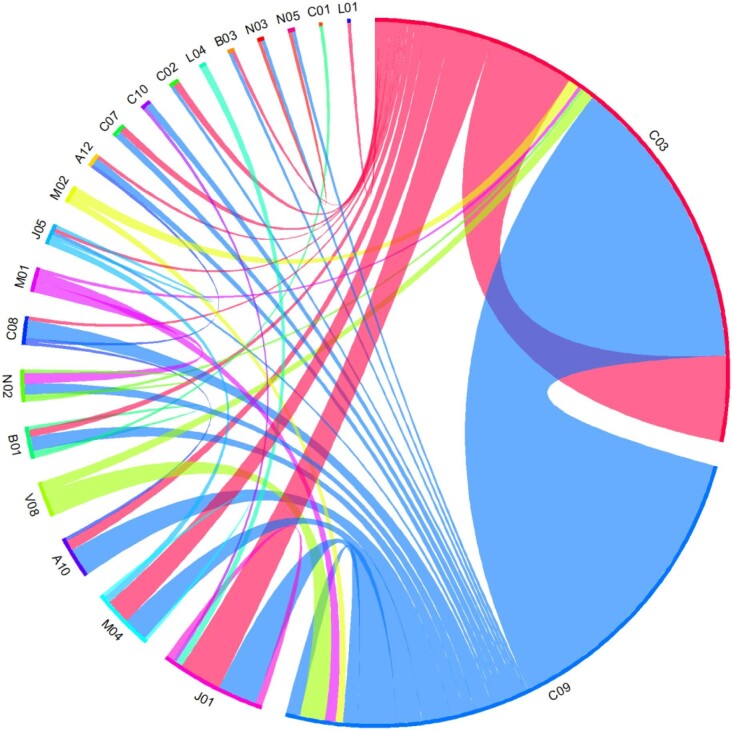
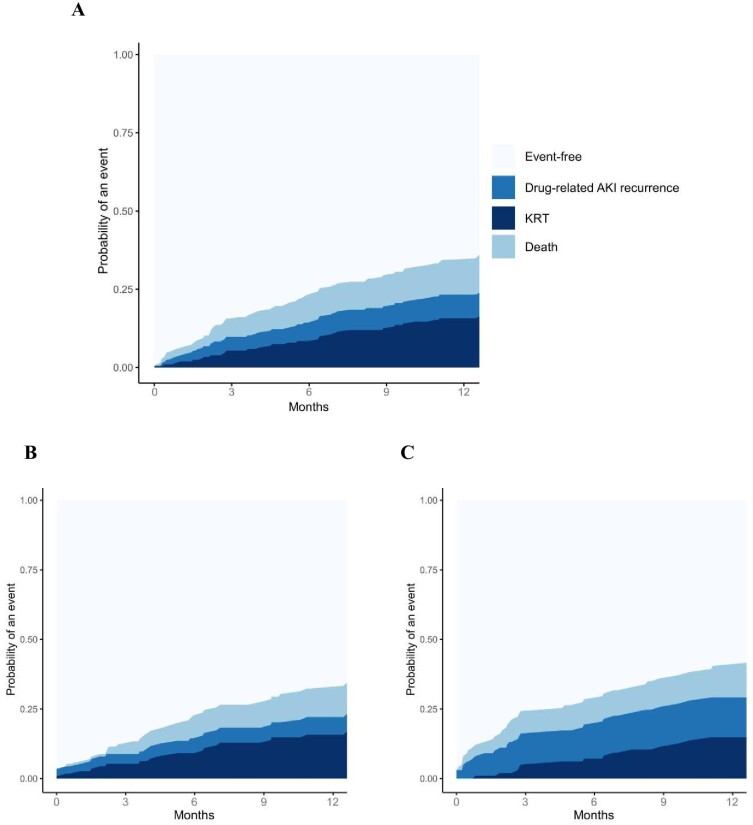
Results: Over a median [interquartile range] period of 4.9 [3.4-5.1] years, 832 cases of AKI were reported in 639 (21%) of the 3033 study participants. The drug-related component associated with AKI accounted for 236 cases, and 28% were judged to be preventable or potentially preventable. The three most frequently implicated drug classes were diuretics, renin-angiotensin system inhibitors, and contrast agents. A history of cardiovascular events, diabetes, lower levels of hemoglobin and eGFR, poor medication adherence, and ≥5 drugs taken daily were associated with a greater risk of drug-related AKI. Full recovery was not attained in 64 (27%) of the 236 cases of drug-related AKI. The 1-year cumulative incidences of recurrence of drug-related AKI, kidney replacement therapy, and death were 7%, 15%, and 11%, respectively, after the first drug-related AKI.
Conclusions: Drug-related AKI is prevalent among patients with CKD. Even though a substantial proportion of these events were classified as stage 1, our findings point to a poor prognosis.
Keywords: acute kidney injury; adverse drug reaction; chronic kidney disease; drugs; pharmacoepidemiology.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
S.M.L., S.L., J.V., V.G.C., and J.M. have nothing to declare. Z.A.M. reports having received grants for CKD-REIN and other research projects from Amgen, Baxter, Fresenius Medical Care, GlaxoSmithKline, Merck Sharp & Dohme-Chibret, Sanofi- Genzyme, Lilly, Otsuka, AstraZeneca, Vifor and the French government, as well as fees and grants to charities from AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline. N.A.P. declare financial support from pharmaceutical companies integrating the public-private partnership of the CKD-REIN cohort: Fresenius Medical Care, GlaxoSmithKline (GSK), Vifor France, and Boeringher Ingelheim; all grants are made to Paris Saclay University.
Figures
References
-
- Kidney Disease: Improving Global, Outcomes (KDIGO) Acute Kidney Injury work group . KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl 2012;2:1–138.
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
