

Atrial Fibrillation and Retinal Stroke
- PMID: 39786774
- PMCID: PMC11718556
- DOI: 10.1001/jamanetworkopen.2024.53819
Atrial Fibrillation and Retinal Stroke
Abstract
Importance: Atrial fibrillation (AF) is the most common, chronic, cardiac arrythmia in older US adults. It is not known whether AF is independently associated with increased risk of retinal stroke (central retinal artery occlusion), a subtype of ischemic stroke that causes severely disabling visual loss in most cases and is a harbinger of further vascular events.
Objective: To determine whether there is an association between AF and retinal stroke.
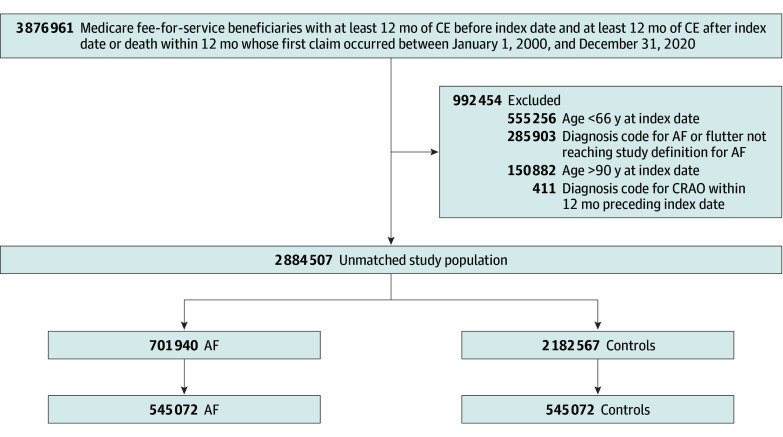
Design, setting, and participants: This retrospective cohort study was performed between July 2023 and May 2024 using computerized inpatient, outpatient, emergency department, and skilled nursing facility claims files for a 5% sample of US fee-for-service Medicare beneficiaries aged 66 years and older between 2000 and 2020. Follow-up ended at death, conclusion of fee-for-service Medicare coverage, end of the study period, or loss to follow-up of 85% of the study cohort.
Exposure: AF, based on validated International Classification of Diseases, Ninth Revision, Clinical Modification and International Statistical Classification of Diseases, Tenth Revision, Clinical Modification diagnosis codes.
Main outcomes and measures: The primary end point was incident retinal stroke in the primary diagnostic position of a single claim in any venue of care. Secondary end points included retinal stroke in any position of a single claim, 1 positive control end point (cerebral ischemic stroke), and 4 negative control end points (central retinal vein occlusion, urinary tract infection, humeral fracture, and cataract). Unadjusted and adjusted hazard ratios (HRs) and rate differences were computed across matched and overlap-weighted cohorts with and without AF (defined as 1 inpatient claim or 2 outpatient claims within a 365-day period).
Results: In total, 1 090 144 patients (591 400 female [54.3%]; mean [SD] age, 76.92 [7.09] years) were included in the study; 545 072 patients had AF and 545 072 were matched controls. The median (IQR) follow-up was 45 (18 to 90) months. In total, 1333 patients with AF (rate, 0.55 per 1000 person-years) and 1082 AF-free matched controls (rate, 0.50 per 1000 person-years) experienced retinal stroke. The cause-specific, adjusted HR of retinal stroke after overlap weighting was 1.14 (95% CI, 1.02 to 1.28; adjusted rate difference, 0.05 [95% CI, -0.01 to 0.11]). AF was associated with cerebral ischemic stroke (adjusted HR, 1.73 [95% CI, 1.69 to 1.76]; adjusted rate difference, 10.11 [95% CI, 9.72 to 10.49]). Of 4 prespecified negative control end points, AF was not associated with central retinal vein occlusion but was associated with urinary tract infection, cataract, and humeral fracture.
Conclusions and relevance: In this cohort study of Medicare beneficiaries aged 66 years and older, AF was independently associated with retinal stroke. The magnitude of the association was small, and a contribution from residual, unmeasured confounding could not be excluded.
Conflict of interest statement
Figures


References
-
- Go AS, Hylek EM, Phillips KA, et al. . Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285(18):2370-2375. doi:10.1001/jama.285.18.2370 - DOI - PubMed
-
- Lamassa M, Di Carlo A, Pracucci G, et al. . Characteristics, outcome, and care of stroke associated with atrial fibrillation in Europe: data from a multicenter multinational hospital-based registry (The European Community Stroke Project). Stroke. 2001;32(2):392-398. doi:10.1161/01.STR.32.2.392 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
