

Tumour deposit count is an independent prognostic factor in colorectal cancer-a population-based cohort study
- PMID: 39787029
- PMCID: PMC11683728
- DOI: 10.1093/bjs/znae309
Tumour deposit count is an independent prognostic factor in colorectal cancer-a population-based cohort study
Erratum in
-
Correction to: Tumour deposit count is an independent prognostic factor in colorectal cancer-a population-based cohort study.Br J Surg. 2025 May 31;112(6):znaf135. doi: 10.1093/bjs/znaf135. Br J Surg. 2025. PMID: 40552947 Free PMC article. No abstract available.
Abstract
Background: Tumour deposits are a prognostic factor for overall survival and distant metastasis in lymph node-negative colorectal cancer. However, the current TNM staging system does not account for the presence of tumour deposits in lymph node-positive colorectal cancer, or for the presence of multiple deposits. This study aimed to investigate the prognostic effect of tumour deposit count in patients with colorectal cancer.
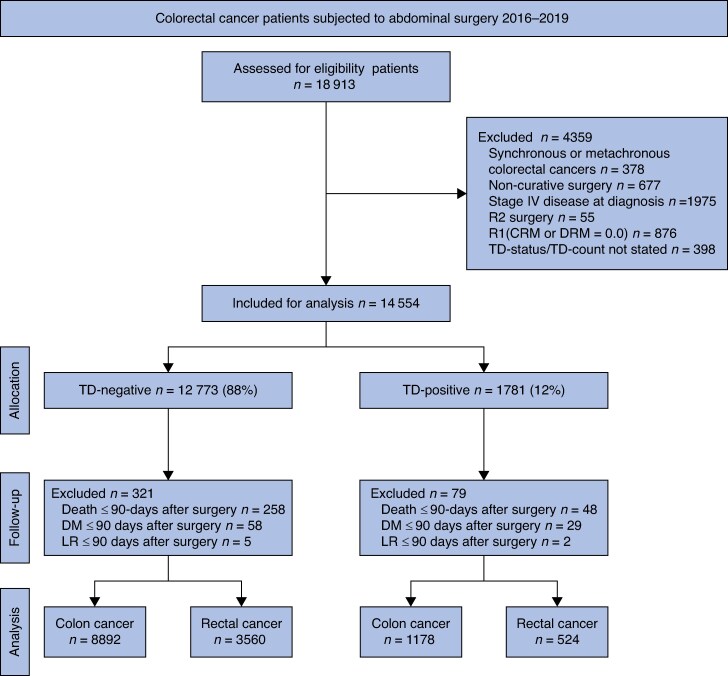
Methods: Patients who underwent curative surgery for colorectal cancer between 2016 and 2019 were identified nationwide from the Swedish Colorectal Cancer Registry. Patients with undisclosed tumour deposit status/count and stage IV disease were excluded. Univariable and multivariable Cox regression analyses were used to assess the prognostic effect of tumour deposit count on overall survival and distant metastasis adjusted for age, sex, neoadjuvant treatment, and number of positive lymph nodes.
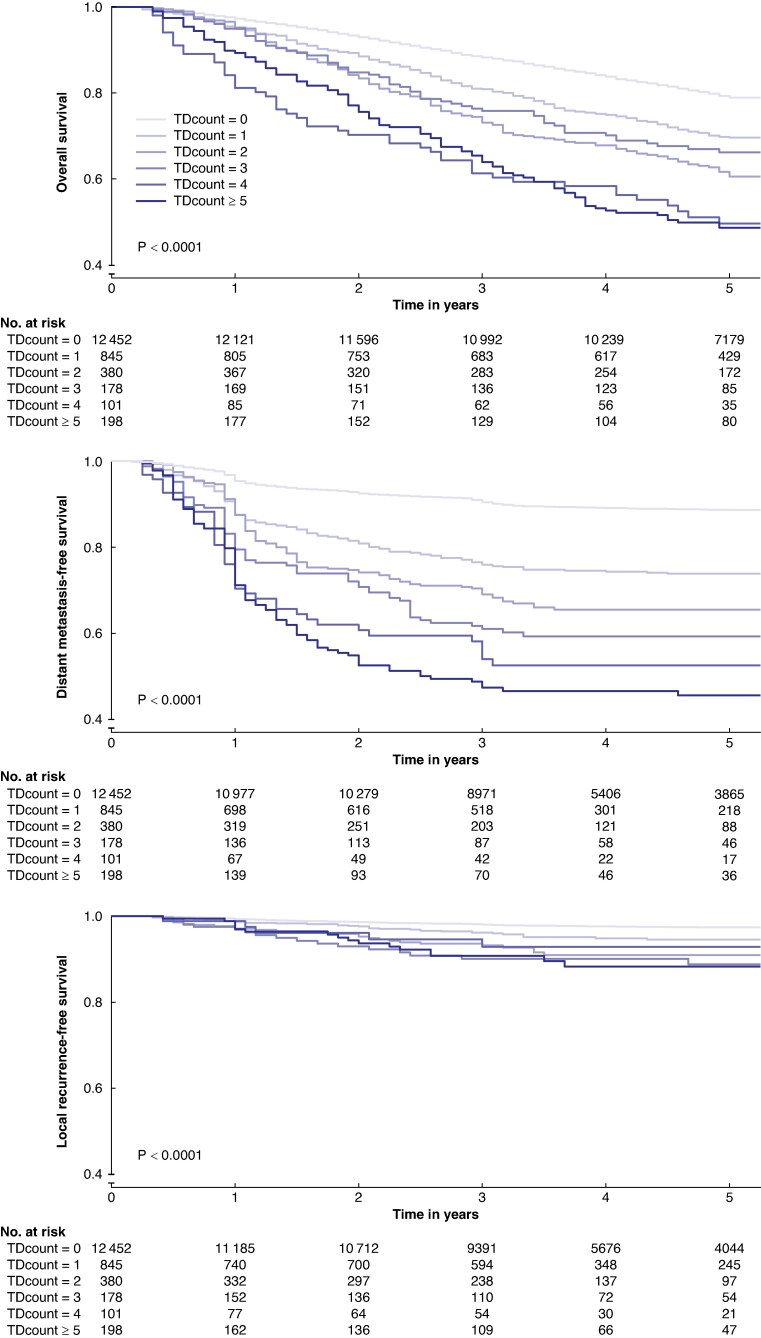
Results: Of 18 913 patients assessed, 14 154 patients were analysed with tumour deposits (TDs) present in 1702 (12%) patients. Patients were stratified by tumour deposit count (0, 1, 2, 3, 4, and ≥5 TDs). Increased tumour deposit count was associated with decreased 5-year overall survival (79%, 70%, 61%, 66%, 50%, 49%) and increased 5-year risk for distant metastasis (14%, 26%, 35%, 41%, 48%, 54%) respectively. Tumour deposit count remained an independent negative prognostic factor after multivariable Cox regression analysis.
Conclusion: Tumour deposit count is a negative prognostic predictor of both overall survival and distant metastasis in colorectal cancer, independent of positive lymph nodes or neoadjuvant treatment. These findings suggest that tumour deposit count should be integrated into the TNM staging regardless of lymph nodes status to improve prognostic accuracy.
Plain language summary
Background: Colorectal cancer, commonly referred to as bowel cancer, is the third most common type of cancer worldwide. Doctors consider various factors when determining the best treatment options and setting realistic expectations for patients. One such factor, called tumour deposits, may be more important than previously recognized.
Aim: This study aimed to investigate whether tumour deposits can help us predict the aggressiveness of an individual’s cancer.
Method: We included data from 14 154 patients who underwent surgery for bowel cancer in Sweden between 2016 and 2019. Using statistical analysis, we examined the relationship between the presence of one or multiple tumour deposits and the risk of serious outcomes, such as cancer recurrence or death.
Findings and conclusion: Our findings indicate that tumour deposits significantly increase the risk of poor outcomes and provide valuable insights beyond current assessments. We believe that considering tumour deposits more thoroughly could lead to improved treatment decisions. However, further research is necessary to identify the most effective treatment strategies for patients with tumour deposits in bowel cancer.
© The Author(s) 2024. Published by Oxford University Press on behalf of BJS Foundation Ltd.
Figures
References
-
- Eileen M, Melina A, Gini A, Lorenzoni V, Cabasag CJ, Mathieu L et al. Global burden of colorectal cancer in 2020 and 2040: incidence and mortality estimates from GLOBOCAN. Gut 2023;72:338–344 - PubMed
-
- Brierley J GM, Wittekind C. TNM Classification of Malignant Tumours (8th edn). Chichester: Wiley-Blackwell, 2017
-
- Sobin LH, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumours (7th edn). Chichester: Wiley-Blackwell, 2009
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
