

Treadmill belt accelerations may not accurately replicate kinematic responses to tripping on an obstacle in older people
- PMID: 39787054
- PMCID: PMC11717211
- DOI: 10.1371/journal.pone.0312261
Treadmill belt accelerations may not accurately replicate kinematic responses to tripping on an obstacle in older people
Abstract
Background: Treadmill belt perturbations have high clinical feasibility for use in perturbation-based training in older people, but their kinematic validity is unclear. This study examined the kinematic validity of treadmill belt accelerations as a surrogate for overground walkway trips during gait in older people.
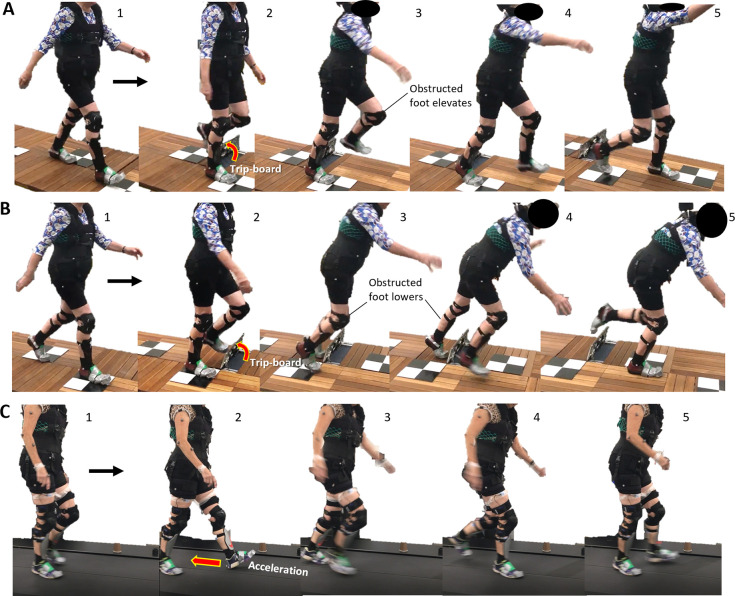
Methods: Thirty-eight community-dwelling older people were exposed to two unilateral belt accelerations (8 m s-2) whilst walking on a split-belt treadmill and two trips induced by a 14 cm trip-board whilst walking on a walkway with condition presentation randomised. Anteroposterior margin of stability (MoS), number of falls, and trunk and lower limb kinematics were quantified for the step prior and five recovery steps following the treadmill perturbations and the walkway trips which elicited elevating and lowering strategies.
Findings: Rates of falls following the treadmill accelerations and walkway trips were 0% and 13.1%, respectively. MoS was similar during the first recovery step (P>0.05) but less negative during subsequent recovery steps following treadmill belt accelerations than walkway trips (P<0.01) regardless of recovery strategy. Excluding the first recovery step in the lowering strategy, recovery step lengths, toe clearance, maximum trunk, hip and knee angles (P<0.05) were smaller during recovery on the treadmill compared to the walkway.
Interpretation: Destabilisation by treadmill belt accelerations quickly dissipated after only one recovery step but continued for multiple recovery steps following walkway trips. Smaller trunk displacement, step lengths, toe clearance and no falls on the treadmill indicate treadmill belt accelerations may not accurately simulate the biomechanical challenge of obstacle-induced trips in older people.
Copyright: © 2025 Jung et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



Similar articles
-
Perturbation-Based Balance Training Using Repeated Trips on a Walkway vs. Belt Accelerations on a Treadmill: A Cross-Over Randomised Controlled Trial in Community-Dwelling Older Adults.Front Sports Act Living. 2021 Aug 20;3:702320. doi: 10.3389/fspor.2021.702320. eCollection 2021. Front Sports Act Living. 2021. PMID: 34490425 Free PMC article.
-
Neuromuscular adaptations to perturbation-based balance training using treadmill belt accelerations do not transfer to an obstacle trip in older people: A cross-over randomised controlled trial.Hum Mov Sci. 2024 Oct;97:103273. doi: 10.1016/j.humov.2024.103273. Epub 2024 Aug 31. Hum Mov Sci. 2024. PMID: 39217920 Clinical Trial.
-
Treadmill induced belt-accelerations may not accurately evoke the muscle responses to obstacle trips in older people.J Electromyogr Kinesiol. 2024 Apr;75:102857. doi: 10.1016/j.jelekin.2024.102857. Epub 2024 Jan 23. J Electromyogr Kinesiol. 2024. PMID: 38330509
-
Provoking Artificial Slips and Trips towards Perturbation-Based Balance Training: A Narrative Review.Sensors (Basel). 2022 Nov 28;22(23):9254. doi: 10.3390/s22239254. Sensors (Basel). 2022. PMID: 36501958 Free PMC article. Review.
-
Meta-analysis on effects of trip-based perturbation training reducing fall risk.Clin Biomech (Bristol). 2025 Apr;124:106470. doi: 10.1016/j.clinbiomech.2025.106470. Epub 2025 Feb 22. Clin Biomech (Bristol). 2025. PMID: 40043478 Review.
References
-
- Australian Institute of Health and Welfare, Injury in Australia: Falls. https://www.aihw.gov.au/reports/injury/falls, 2022 (accessed 30 November 2022).
-
- Menant J.C., St George R.J., Fitzpatrick R.C., Lord S.R., Impaired depth perception and restricted pitch head movement increase obstacle contacts when dual-tasking in older people, Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences 65(7) (2010) 751–757. doi: 10.1093/gerona/glq015 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
