

Trastuzumab-Pertuzumab Plus Eribulin or Taxane as First-Line Chemotherapy for Human Epidermal Growth Factor 2-Positive Locally Advanced/Metastatic Breast Cancer: The Randomized Noninferiority Phase III EMERALD Trial
- PMID: 39787453
- PMCID: PMC11974627
- DOI: 10.1200/JCO-24-01888
Trastuzumab-Pertuzumab Plus Eribulin or Taxane as First-Line Chemotherapy for Human Epidermal Growth Factor 2-Positive Locally Advanced/Metastatic Breast Cancer: The Randomized Noninferiority Phase III EMERALD Trial
Abstract
Purpose: Trastuzumab-pertuzumab (HP) plus taxane is a current standard first-line therapy for recurrent or metastatic human epidermal growth factor 2 (HER2)+ breast cancer (BC). We investigated noninferiority of eribulin to a taxane when combined with dual HER2 blockade as first-line systemic treatment for locally advanced/metastatic HER2+ BC.
Methods: In the phase III EMERALD trial (target sample size, 480; ClinicalTrials.gov identifier: NCT03264547/UMIN000027938), patients were randomly assigned (1:1) to receive eribulin 1.4 mg/m2 once daily on days 1 and 8 (eribulin group) or a taxane (docetaxel 75 mg/m2 once on day 1 or paclitaxel 80 mg/m2 once daily on days 1, 8, and 15; taxane group) intravenously in a 21-day cycle, each with HP on day 1. The primary end point was progression-free survival (PFS; intention-to-treat population). Secondary end points included objective response rate, overall survival (OS), patient-reported quality of life (QoL), and safety. Noninferiority was tested using the stratified Cox proportional hazards model to estimate hazard ratios (HRs) for PFS events, with a noninferiority HR margin of 1.33.
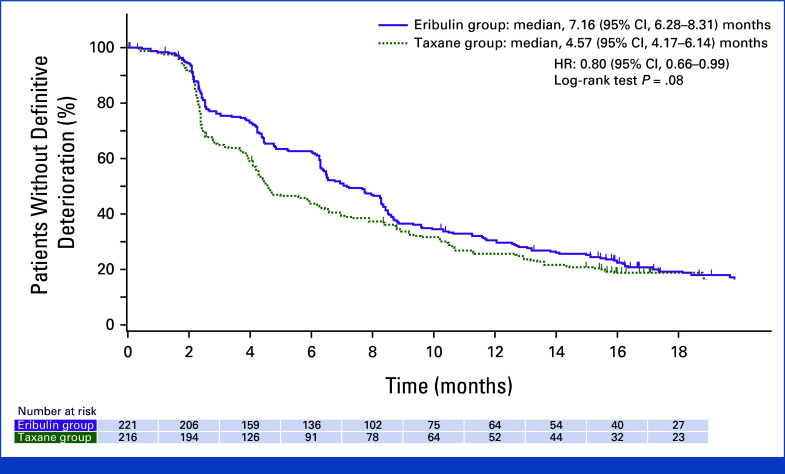
Results: Between August 2017 and June 2021, 446 patients (median age, 56.0 years) were enrolled. The median PFS was 14.0 and 12.9 months in the eribulin group (n = 224) and taxane group (n = 222 [docetaxel/paclitaxel, n = 186/36]), respectively (HR, 0.95 [95% CI, 0.76 to 1.19]), which confirmed the noninferiority of the study regimen. The median OS was 65.3 months in the taxane group but has not been reached in the eribulin group. Median time to QoL deterioration was numerically longer with eribulin than with taxane. Adverse event (AE) rates were similar, despite the longer duration of eribulin use. Infusion reaction, skin-related AEs, diarrhea, and edema were more common with taxane, whereas neutropenia was more common with eribulin.
Conclusion: The results suggested that eribulin + HP is an option for first-line treatment of locally advanced/metastatic HER2+ BC.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures




References
-
- Wolff AC, Hammond MEH, Hicks DG, et al. : Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol 31:3997-4013, 2013 - PubMed
-
- Chang E, Mougalian SS, Adelson KB, et al. : Association between prolonged metastatic free interval and recurrent metastatic breast cancer survival: Findings from the SEER database. Breast Cancer Res Treat 173:209-216, 2019 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
