

Effectiveness of shared decision making strategies for stroke prevention among patients with atrial fibrillation: cluster randomized controlled trial
- PMID: 39788611
- PMCID: PMC11713231
- DOI: 10.1136/bmj-2024-079976
Effectiveness of shared decision making strategies for stroke prevention among patients with atrial fibrillation: cluster randomized controlled trial
Abstract
Objective: To evaluate the effectiveness of multiple decision aid strategies in promoting high quality shared decision making for prevention of stroke in patients with non-valvular atrial fibrillation.
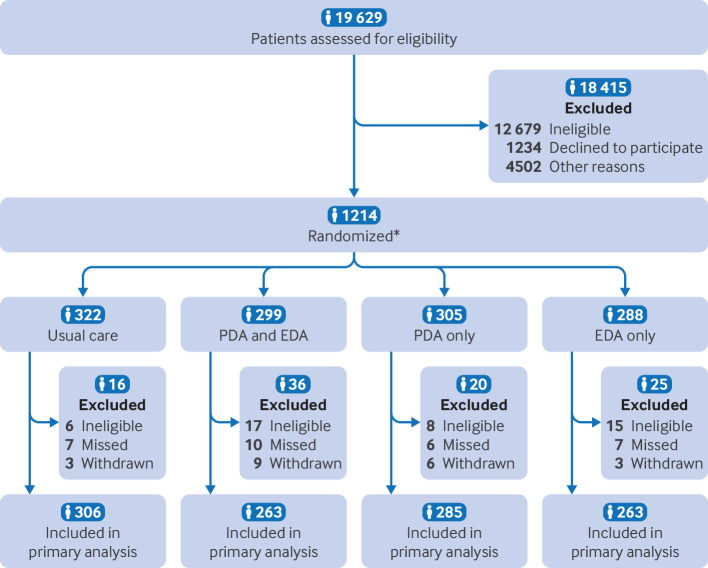
Design: Cluster randomized controlled trial.
Setting: Six academic medical centers in the United States.
Participants: Patient participants were aged ≥18 with a diagnosis of non-valvular atrial fibrillation, at risk for stroke (CHA2DS2-VASc ≥1 for men, ≥2 for women), and scheduled for a clinical appointment to discuss stroke prevention strategies. Participating clinicians were those who manage stroke prevention strategies for participating patients.
Intervention: Patients were randomized to use a patient decision aid or usual care; clinicians were randomized to use an encounter decision aid or usual care with all participating patients.
Main outcome measures: Primary outcome measures were quality of shared decision making measured by OPTION12, knowledge of atrial fibrillation and its management, and decisional conflict.
Results: 1117 participants across six sites were included in the analysis. Compared with usual care, the combined use of both the patient decision aid and the encounter decision aid improved the quality of shared decision making (adjusted mean difference 12.1 (95% confidence interval (CI) 8.0 to 16.2; P<0.001), improved patients' knowledge (odds ratio 1.68 (95% CI 1.35 to 2.09; P<0.001), and reduced patients' decisional conflict (adjusted mean difference -6.3 (95% CI -9.6 to -3.1; P<0.001). Statistically significant improvements were also observed with the encounter decision aid alone versus usual care for all three outcomes and with the patient decision aid alone versus usual care for quality of shared decision making and knowledge. No important differences were observed in treatment choices for stroke prevention or in participants' satisfaction. No statistically significant difference in the length of visit across study groups was detected.
Conclusion: Patients who received any decision aid (encounter decision aid, patient decision aid, or both) had lower decisional conflict, better shared decision making, and greater knowledge than those receiving no decision aid, except for the effect of the patient decision aid on decisional conflict, which did not reach statistical significance. The study establishes that use of either pre-visit or in-visit decision aids individually or in combination is advantageous compared with usual care.
Trial registration: ClinicalTrials.gov NCT04357288.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest and declare: support from the American Heart Association and the Patient-Centered Outcomes Research Institute for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures


Similar articles
-
Assessment of Shared Decision-making for Stroke Prevention in Patients With Atrial Fibrillation: A Randomized Clinical Trial.JAMA Intern Med. 2020 Sep 1;180(9):1215-1224. doi: 10.1001/jamainternmed.2020.2908. JAMA Intern Med. 2020. PMID: 32897386 Free PMC article. Clinical Trial.
-
Personalized, Electronic Health Record-Integrated Decision Aid for Stroke Prevention in Atrial Fibrillation: A Small Cluster Randomized Trial and Qualitative Analysis of Efficacy and Acceptability.Circ Cardiovasc Qual Outcomes. 2021 Jun;14(6):e007329. doi: 10.1161/CIRCOUTCOMES.120.007329. Epub 2021 Jun 10. Circ Cardiovasc Qual Outcomes. 2021. PMID: 34107740 Clinical Trial.
-
Shared decision making for stroke prevention in atrial fibrillation: study protocol for a randomized controlled trial.Trials. 2017 Sep 29;18(1):443. doi: 10.1186/s13063-017-2178-y. Trials. 2017. PMID: 28962662 Free PMC article. Clinical Trial.
-
Shared Decision Making Tools for People Facing Stroke Prevention Strategies in Atrial Fibrillation: A Systematic Review and Environmental Scan.Med Decis Making. 2021 Jul;41(5):540-549. doi: 10.1177/0272989X211005655. Epub 2021 Apr 24. Med Decis Making. 2021. PMID: 33896270 Free PMC article.
-
Use of digital patient decision-support tools for atrial fibrillation treatments: a systematic review and meta-analysis.BMJ Evid Based Med. 2025 Jan 22;30(1):10-21. doi: 10.1136/bmjebm-2023-112820. BMJ Evid Based Med. 2025. PMID: 38950915 Free PMC article.
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017;135:e146-603. 10.1161/CIR.0000000000000485 - DOI - PMC - PubMed
-
- Reiffel JA. Atrial fibrillation and stroke: epidemiology. Am J Med 2014;127:e15-6. - PubMed
-
- Hindricks G, Potpara T, Dagres N, et al. ESC Scientific Document Group . 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2021;42:373-498. 10.1093/eurheartj/ehaa612 - DOI - PubMed
-
- January CT, Wann LS, Alpert JS, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2014;64:e1-76. 10.1016/j.jacc.2014.03.022 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical