

Comparing acute versus AIDS ART initiation on HIV-1 integration sites and clonal expansion
- PMID: 39788938
- PMCID: PMC11718275
- DOI: 10.1038/s41392-024-02113-7
Comparing acute versus AIDS ART initiation on HIV-1 integration sites and clonal expansion
Abstract
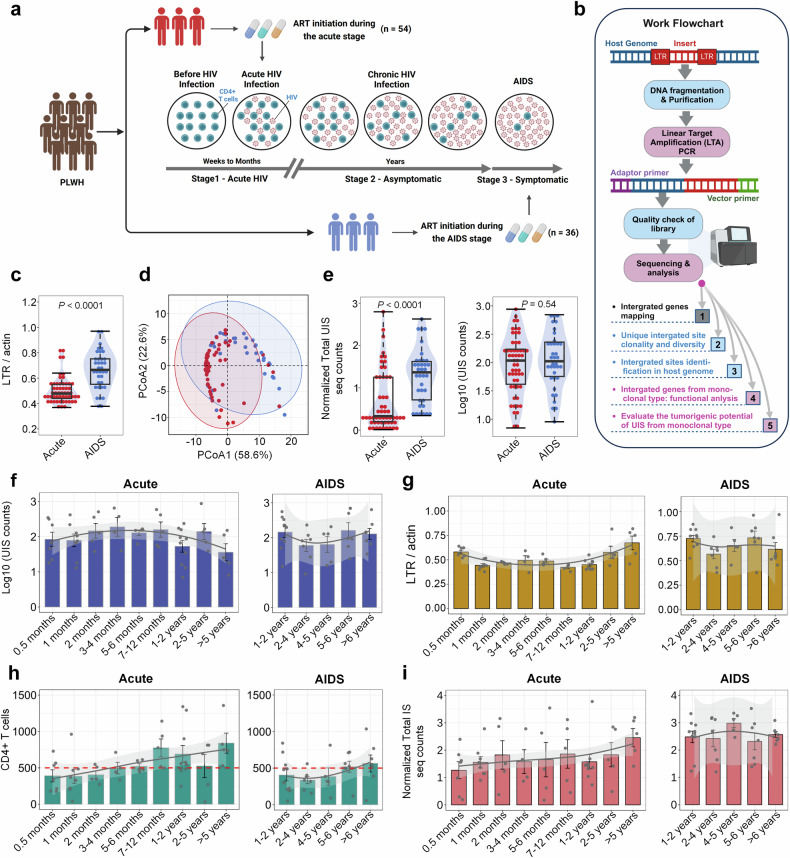
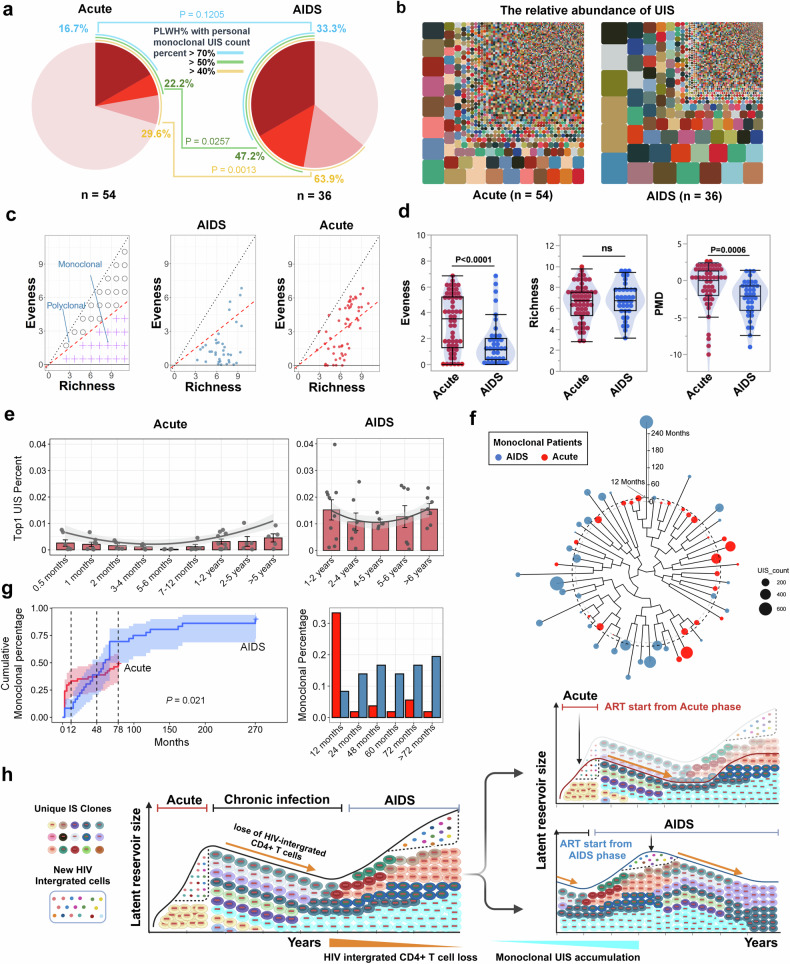
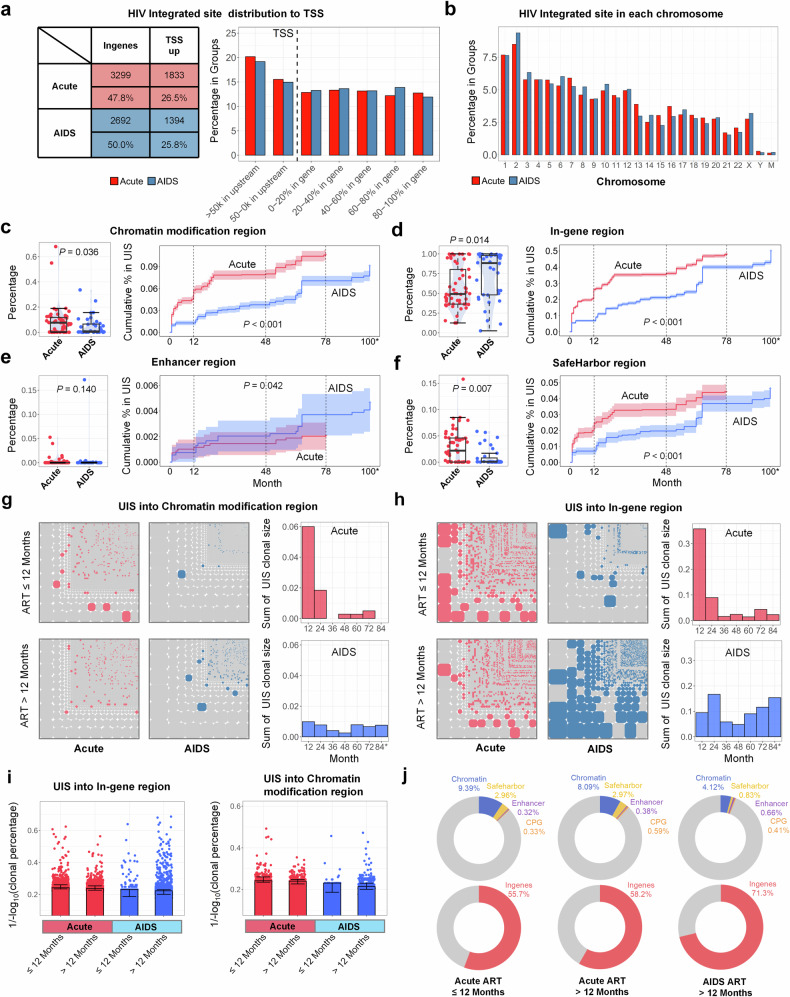
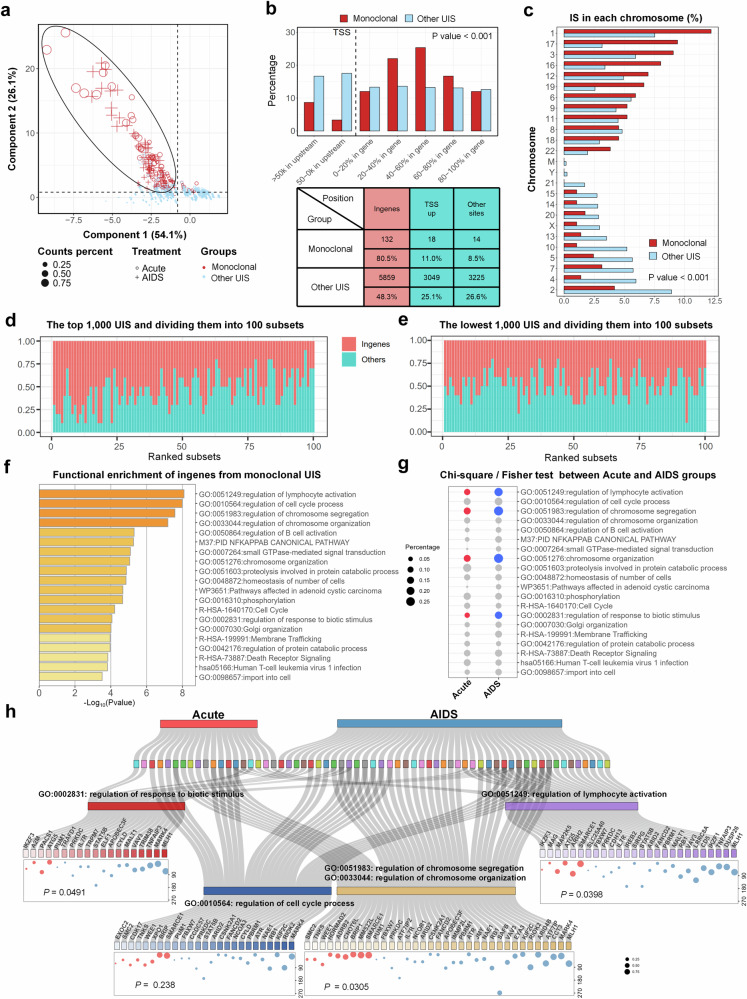
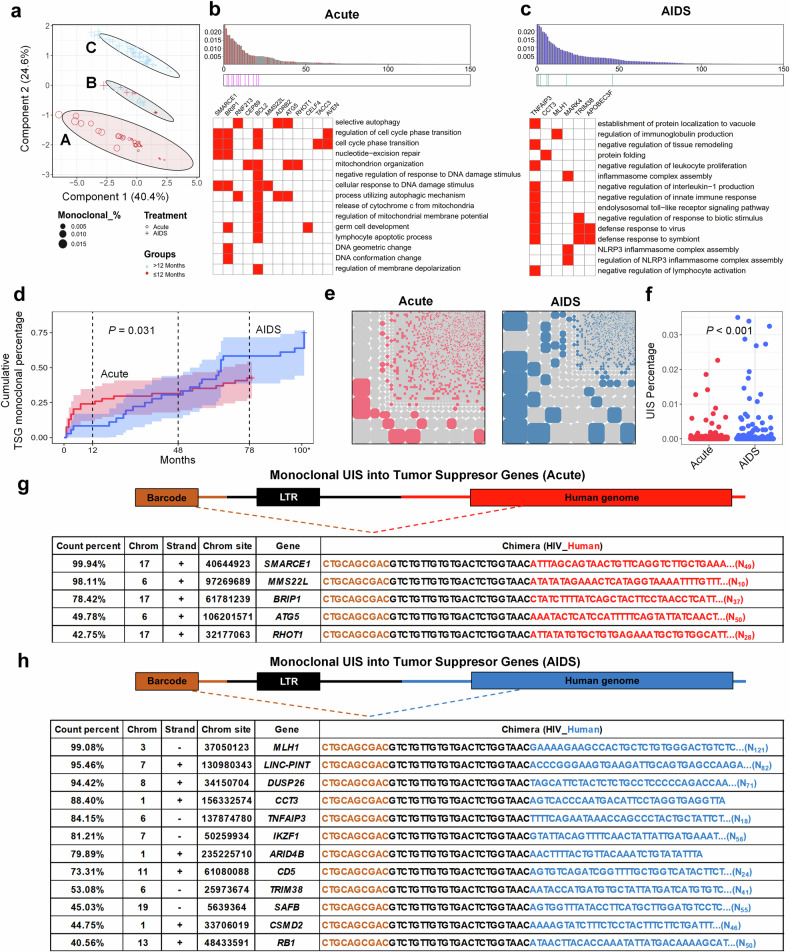
Early antiretroviral therapy (ART) initiation is known to limit the establishment of the HIV reservoir, with studies suggesting benefits such as a reduced number of infected cells and a smaller latent reservoir. However, the long-term impact of early ART initiation on the dynamics of the infected cell pool remains unclear, and clinical evidence directly comparing proviral integration site counts between early and late ART initiation is limited. In this study, we used Linear Target Amplification-PCR (LTA-PCR) and Next Generation Sequencing to compare unique integration site (UIS) clonal counts between individuals who initiated ART during acute HIV infection stage (Acute-ART group) and those in the AIDS stage (AIDS-ART group). Our analysis revealed distinct clonal distribution patterns, with greater UIS heterogeneity in Acute-ART group and more homogeneity in AIDS-ART group. Monoclonal UIS accumulation, predominantly in-gene regions, was influenced by ART timing and duration, with early treatment delaying this process. Host cell genes integrated by HIV provirus as monoclonal types were enriched in cell cycle and lymphocyte activation pathways. Tumor suppressor genes (TSGs) were more frequently integrated as monoclonal types in AIDS-ART group, suggesting potential risk factors. Overall, we introduced a sequencing method to assess provirus size in human peripheral blood and identified the widespread presence of monoclonal distribution of UIS in AIDS-ART group after long-term treatment. The early intervention helps slow the progress of clonal expansion of infected cells, reducing the formation of stable and persistent reservoirs, and ultimately posing fewer barriers to achieving a functional cure.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Intact HIV Proviruses Persist in Children Seven to Nine Years after Initiation of Antiretroviral Therapy in the First Year of Life.J Virol. 2020 Jan 31;94(4):e01519-19. doi: 10.1128/JVI.01519-19. Print 2020 Jan 31. J Virol. 2020. PMID: 31776265 Free PMC article.
-
Antigen specificities and proviral integration sites differ in HIV-infected cells by timing of antiretroviral treatment initiation.J Clin Invest. 2024 Jun 4;134(14):e159569. doi: 10.1172/JCI159569. J Clin Invest. 2024. PMID: 38833307 Free PMC article.
-
Early Emergence and Long-Term Persistence of HIV-Infected T-Cell Clones in Children.mBio. 2021 Apr 8;12(2):e00568-21. doi: 10.1128/mBio.00568-21. mBio. 2021. PMID: 33832973 Free PMC article.
-
The role of integration and clonal expansion in HIV infection: live long and prosper.Retrovirology. 2018 Oct 23;15(1):71. doi: 10.1186/s12977-018-0448-8. Retrovirology. 2018. PMID: 30352600 Free PMC article. Review.
-
The Clonal Expansion Dynamics of the HIV-1 Reservoir: Mechanisms of Integration Site-Dependent Proliferation and HIV-1 Persistence.Viruses. 2021 Sep 17;13(9):1858. doi: 10.3390/v13091858. Viruses. 2021. PMID: 34578439 Free PMC article. Review.
Cited by
-
Association between baseline HIV-1 DNA levels and clinical outcomes in people living with HIV: a meta-analysis of cohort studies.Emerg Microbes Infect. 2025 Dec;14(1):2508759. doi: 10.1080/22221751.2025.2508759. Epub 2025 May 28. Emerg Microbes Infect. 2025. PMID: 40387837 Free PMC article.
-
Circulating Biomarker Panorama in HIV-Associated Lymphoma: A Bridge from Early Risk Warning to Prognostic Stratification.Biomolecules. 2025 Jul 11;15(7):993. doi: 10.3390/biom15070993. Biomolecules. 2025. PMID: 40723865 Free PMC article. Review.
References
-
- Leth, S. et al. Combined effect of Vacc-4x, recombinant human granulocyte macrophage colony-stimulating factor vaccination, and romidepsin on the HIV-1 reservoir (REDUC): a single-arm, phase 1B/2A trial. Lancet HIV3, e463–e472 (2016). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
