

Efficacy of laparoscopic cardiectomy combined with side overlap anastomosis for the treatment of terminal achalasia
- PMID: 39789050
- PMCID: PMC11718196
- DOI: 10.1038/s41598-024-74143-8
Efficacy of laparoscopic cardiectomy combined with side overlap anastomosis for the treatment of terminal achalasia
Abstract
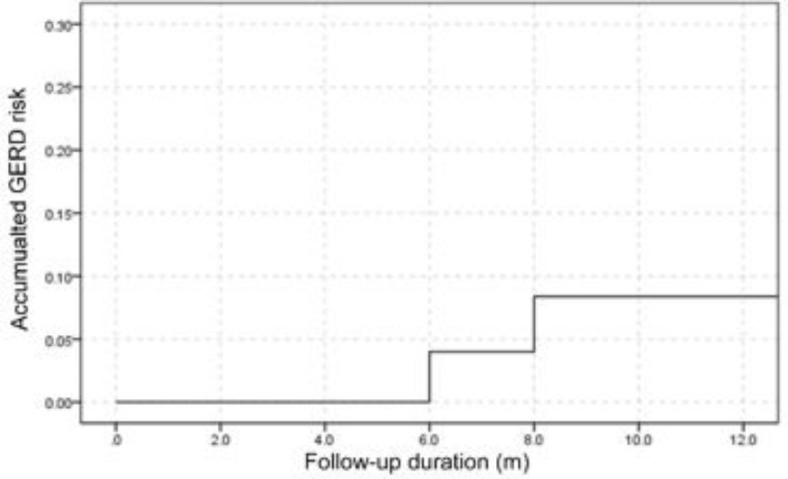
To investigate the safety and short-term effectiveness of laparoscopic-assisted cardiectomy with side-overlap esophagogastric reconstruction for the treatment of terminal or end-stage achalasia, patients with end-stage achalasia treated with laparoscopic-assisted cardiectomy with side-overlap esophagogastric reconstruction were retrospectively enrolled. The clinical data, surgical data and follow-up were analyzed. Among twenty-five patients enrolled, the achalasia type St was present in 12 (48%) patients, type Sg in 9 (36%), and type aSg in 4 (16%). The surgical time ranged 60-180 min (median 100 min) with an intraoperative blood loss 20-200 ml (median 50 ml). Five (20%) patients experienced complications within a week after surgery, with fever (> 38.5 ℃) in two (40%) patients within 3 days after surgery, abdominal incision infection in one (20%), and anastomotic leak in two (40%). The postoperative hospitalization time ranged 8-44 (median 10) days. Follow-up was conducted 6-38 months (median 16) after surgery. Compared with the preoperative Eckardt score (7.64 ± 1.32), the Eckardt score was significantly (P < 0.01) decreased at one month (0.52 ± 0.87), 6 (0.84 ± 1.11) and 12 (1.23 ± 1.23) months after surgery in all patients. The Eckardt score in type St was significantly (P < 0.05) smaller than in type Sg or aSg at 6 and 12 months after surgery. Seven patients maintained an Eckardt score 0 with complete relief of their symptoms. The effective rate was 100% for type St, 88.8% for type Sg, and 75% for type aSg. The effective rates at 1 month, 6 and 12 months after surgery were 100% (95% CI: 100% -100%), 96% (95% CI: 87.7 -100%), and 92% (95% CI: 80.6 -100%). Two patients were diagnosed with gastroesophageal reflux disease (GERD) at the end of the follow-up. The cumulative incidence of GERD at 1 month, 6 and 12 months after surgery was 0, 4% (95% confidence interval or CI: 0-12.3%), and 8% (95% CI: 0-19.4%). In conclusion, the laparoscopic-assisted cardiectomy with side-overlap esophagogastric reconstruction is safe and effective for the treatment of end-stage achalasia, and the effect is significantly better for achalasia type St than for types Sg and aSg.
Keywords: Achalasia; Effectiveness; End stage; Laparoscopic-assisted cardiectomy; Side-overlap esophagogastric reconstruction.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Comparison of clinical efficacy between modified Kamikawa anastomosis in laparoscopic proximal gastrectomy and Roux-en-Y anastomosis in laparoscopic total gastrectomy.Sci Rep. 2024 Jul 26;14(1):17181. doi: 10.1038/s41598-024-68514-4. Sci Rep. 2024. PMID: 39060330 Free PMC article.
-
[Comparison of short-term safety of two anastomotic techniques when resecting Siewert type II adenocarcinoma of the esophagogastric junction: a multicenter retrospective cohort study].Zhonghua Wei Chang Wai Ke Za Zhi. 2024 Jan 25;27(1):47-53. doi: 10.3760/cma.j.cn441530-20230913-00088. Zhonghua Wei Chang Wai Ke Za Zhi. 2024. PMID: 38262900 Chinese.
-
Per Oral Endoscopic Myotomy (POEM) for pediatric achalasia: Institutional experience and outcomes.J Pediatr Surg. 2022 Nov;57(11):728-735. doi: 10.1016/j.jpedsurg.2022.02.017. Epub 2022 Feb 25. J Pediatr Surg. 2022. PMID: 35361482
-
Achalasia: laparoscopic Heller myotomy with fundoplication versus peroral endoscopic myotomy-a systematic review and meta-analysis.Esophagus. 2024 Jul;21(3):298-305. doi: 10.1007/s10388-024-01063-x. Epub 2024 May 22. Esophagus. 2024. PMID: 38775883 Free PMC article.
-
Controversies in the treatment of gastroesophageal reflux and achalasia.World J Gastroenterol. 2006 May 28;12(20):3155-61. doi: 10.3748/wjg.v12.i20.3155. World J Gastroenterol. 2006. PMID: 16718833 Free PMC article. Review.
References
-
- Boeckxstaens, G. et al. 10-year follow-up results of the European achalasia trial: a multicentre randomised controlled trial comparing pneumatic dilation with laparoscopic heller myotomy. Gut. 73, 582–589 (2024). - PubMed
-
- Delgado-Miguel, C., Amarnath, R. P. & Camps, J. I. Robotic-assisted vs. laparoscopic heller’s myotomy for achalasia in children. J. Pediatr. Surg. 59, 1072–1076 (2024). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
