

Hemoglobin glycation index and mortality risk in metabolic dysfunction-associated steatotic liver disease patients: a novel U-shaped association
- PMID: 39789085
- PMCID: PMC11718243
- DOI: 10.1038/s41598-024-82034-1
Hemoglobin glycation index and mortality risk in metabolic dysfunction-associated steatotic liver disease patients: a novel U-shaped association
Abstract
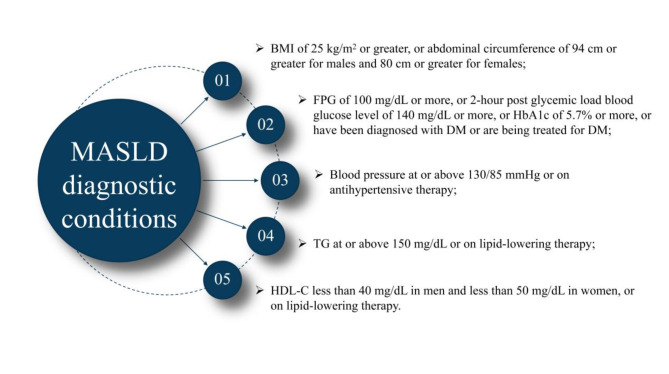
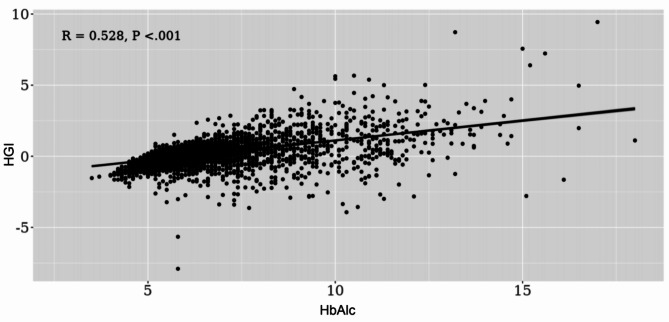
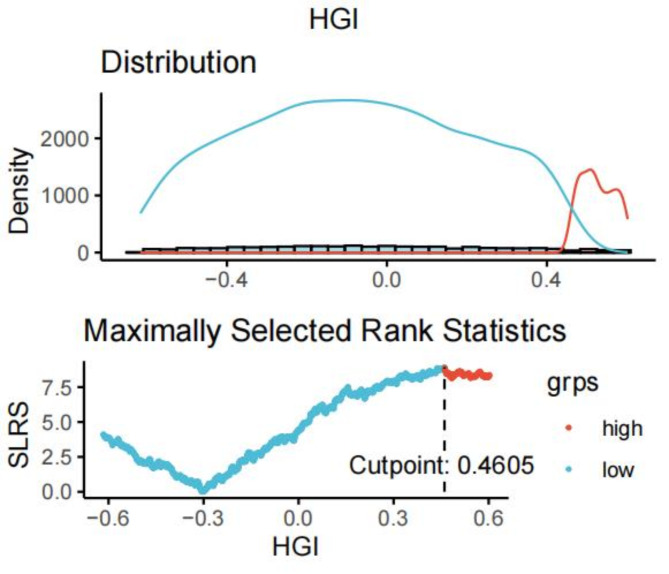
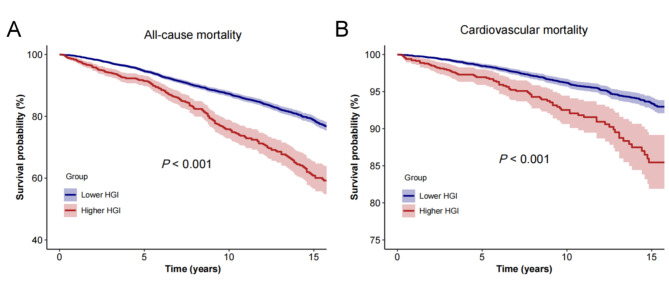
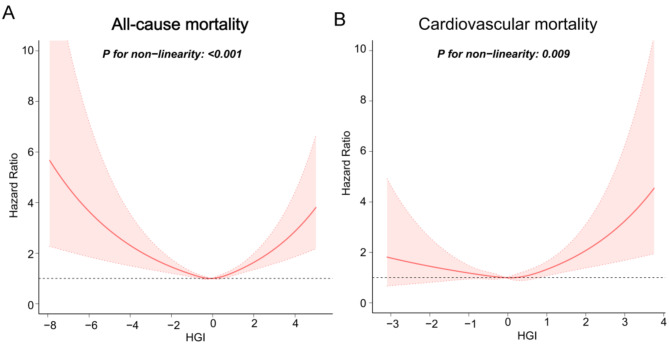
Identifying dependable prognostic indicators is essential for the efficient management of metabolic dysfunction-associated steatotic liver disease (MASLD). The index of hemoglobin glycation (HGI) has been demonstrated to be closely linked to the onset and advancement of MASLD. Currently, no studies have investigated the relationship between HGI and mortality rates among MASLD patients. This study analyzed data from the National Health and Nutrition Examination Surveys (NHANES) covering 1999 to 2018, involving 8,257 adult patients diagnosed with MASLD. The HGI was determined using a linear regression model that correlated hemoglobin A1c (HbA1c) with fasting plasma glucose (FPG). The study employed Kaplan-Meier survival curves and weighted Cox proportional hazards models to evaluate the independent association between HGI and mortality risk. The study utilized restricted cubic splines (RCS) to visually depict the relationship between HGI and mortality risk. Over a median follow-up duration of 97.0 months, there were 1,352 recorded deaths, among which 386 were attributed to cardiovascular disease (CVD). Participants were classified into two groups based on their HGI values: the high HGI group (≥ 0.4605) and the low HGI group (< 0.4605). The results from the weighted Cox proportional hazards model indicated that individuals in the high HGI group faced a significantly higher risk of all-cause mortality (HR 1.47, 95% CI 1.19-1.82, P < 0.001). However, no significant increase in CVD mortality risk was observed (HR 1.38, 95% CI 0.95-1.99, P = 0.090). The RCS analysis identified a U-shaped association between HGI and both all-cause mortality and CVD mortality, with critical points at -0.0564 and - 0.0573, respectively. Below the critical points, HGI was negatively correlated with all-cause mortality (HR 0.82, 95% CI: 0.72-0.92, P < 0.001) and not significantly associated with CVD mortality (HR 0.78, 95% CI: 0.57-1.07, P = 0.126). Above the critical points, HGI was significantly positively correlated with both all-cause mortality (HR 1.36, 95% CI: 1.20-1.53, P < 0.001) and CVD mortality (HR 1.44, 95% CI: 1.11-1.88, P = 0.007). Further subgroup and interaction analyses corroborated the reliability of these findings. HGI could potentially function as a useful and dependable marker for evaluating all-cause mortality and cardiovascular mortality in MASLD patients.
Keywords: All-cause mortality; Cardiovascular mortality; HGI; MASLD.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics approval and consent to participate: The research received clearance from the National Center for Health Statistics (NCHS) Research Ethics Review Committee. Each participant provided written consent prior to engagement in the study.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
