

Prospective validation of ORACLE, a clonal expression biomarker associated with survival of patients with lung adenocarcinoma
- PMID: 39789179
- PMCID: PMC11779643
- DOI: 10.1038/s43018-024-00883-1
Prospective validation of ORACLE, a clonal expression biomarker associated with survival of patients with lung adenocarcinoma
Abstract
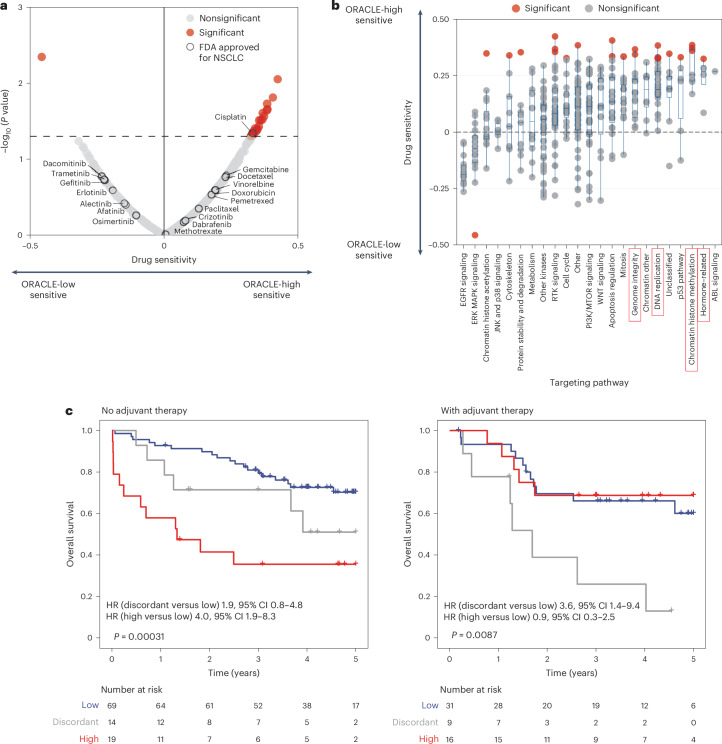
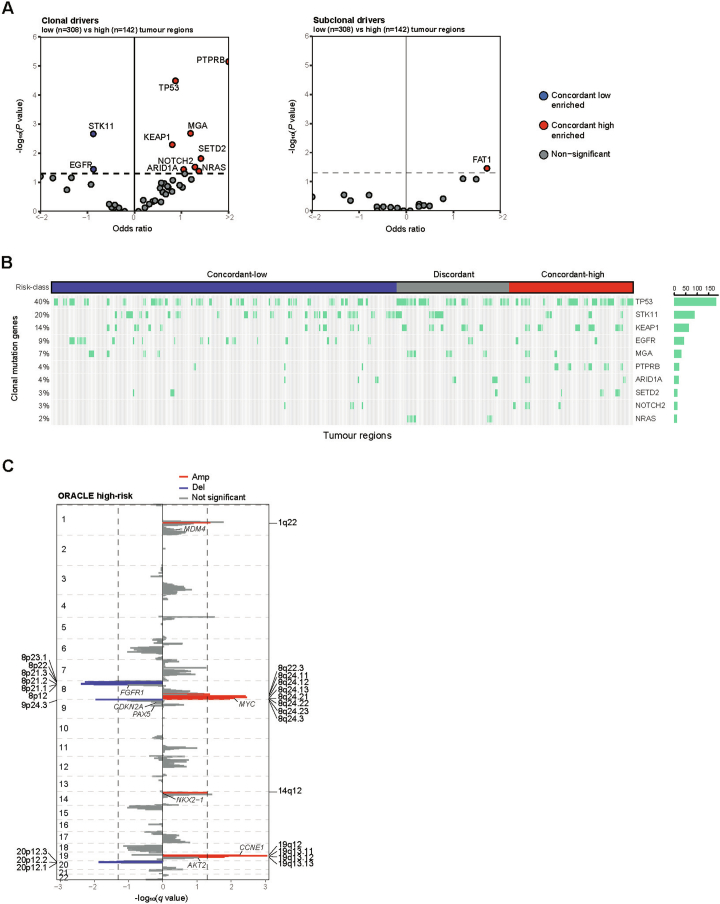
Human tumors are diverse in their natural history and response to treatment, which in part results from genetic and transcriptomic heterogeneity. In clinical practice, single-site needle biopsies are used to sample this diversity, but cancer biomarkers may be confounded by spatiogenomic heterogeneity within individual tumors. Here we investigate clonally expressed genes as a solution to the sampling bias problem by analyzing multiregion whole-exome and RNA sequencing data for 450 tumor regions from 184 patients with lung adenocarcinoma in the TRACERx study. We prospectively validate the survival association of a clonal expression biomarker, Outcome Risk Associated Clonal Lung Expression (ORACLE), in combination with clinicopathological risk factors, and in stage I disease. We expand our mechanistic understanding, discovering that clonal transcriptional signals are detectable before tissue invasion, act as a molecular fingerprint for lethal metastatic clones and predict chemotherapy sensitivity. Lastly, we find that ORACLE summarizes the prognostic information encoded by genetic evolutionary measures, including chromosomal instability, as a concise 23-transcript assay.
Trial registration: ClinicalTrials.gov NCT01888601.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: D.B. reports personal fees from NanoString and AstraZeneca and has a patent PCT/GB2020/050221 issued on methods for cancer prognostication. Y.W. consults for E15 VC and Prokarium. D.A.M. reports speaker fees from AstraZeneca, Eli Lilly, BMS and Takeda, consultancy fees from AstraZeneca, Thermo Fisher, Takeda, Amgen, Janssen, MIM Software, Bristol Myers Squibb and Eli Lilly and has received educational support from Takeda and Amgen. S.C.T. has acted as a consultant for Revolution Medicines. J.D. has acted as a consultant for AstraZeneca, Jubilant, Theras, Roche and Vividion and has funded research agreements with Bristol Myers Squibb, Revolution Medicines, Novartis, Vividion and AstraZeneca. M.J.-H. has consulted for Astex Pharmaceutical and Achilles Therapeutics, and is a member of, the Achilles Therapeutics Scientific Advisory Board and Steering Committee, has received speaker honoraria from Pfizer, Astex Pharmaceuticals, Oslo Cancer Cluster, Bristol Myers Squibb and Genentech. M.J.-H. is listed as a co-inventor on a European patent application relating to methods to detect lung cancer PCT/US2017/028013), this patent has been licensed to commercial entities and, under terms of employment, M.J.-H. is due a share of any revenue generated from such license(s), and is also listed as a co-inventor on the GB priority patent application (GB2400424.4) with title: Treatment and Prevention of Lung Cancer. N.J.B. is listed as a co-inventor on a patent to identify responders to cancer treatment (PCT/GB2018/051912), has a patent application (PCT/GB2020/050221) on methods for cancer prognostication and a patent on methods for predicting anti-cancer response (US14/466,208). C.S. acknowledges grant support from AstraZeneca, Boehringer-Ingelheim, BMS, Pfizer, Roche-Ventana, Invitae (previously Archer Dx (collaboration in minimal residual disease sequencing technologies)) and Ono Pharmaceutical. C.S. is an AstraZeneca Advisory Board member and Chief Investigator for the AZ MeRmaiD 1 and 2 clinical trials and is also Co-Chief Investigator of the NHS Galleri trial funded by GRAIL and a paid member of GRAIL’s SAB. He receives consultant fees from Achilles Therapeutics (also a SAB member), Bicycle Therapeutics (also a SAB member), Genentech, Medicxi, Roche Innovation Centre–Shanghai, Metabomed (until July 2022), and the Sarah Cannon Research Institute. C.S. had stock options in Apogen Biotechnologies and GRAIL until June 2021, currently has stock options in Epic Bioscience and Bicycle Therapeutics and has stock options and is co-founder of Achilles Therapeutics. C.S. is an inventor on a European patent application relating to an assay technology to detect tumor recurrence (PCT/ GB2017/053289), the patent has been licensed to commercial entities and under his terms of employment, C.S. is due a revenue share of any revenue generated from such license(s). C.S. holds patents relating to targeting neoantigens (PCT/EP2016/059401), identifying patient responses to immune checkpoint blockade (PCT/EP2016/071471), determining HLA LOH (PCT/ GB2018/052004), predicting survival rates of patients with cancer (PCT/GB2020/050221), identifying patients who respond to cancer treatment (PCT/GB2018/051912), a US patent relating to detecting tumor mutations (PCT/US2017/28013), methods for lung cancer detection (US20190106751A1) and both a European and US patent related to identifying indel mutation targets (PCT/GB2018/051892) and is a co-inventor on a patent application to determine methods and systems for tumor monitoring (PCT/EP2022/077987). C.S. is a named inventor on a provisional patent related to a ctDNA detection algorithm. The other authors declare no competing interests.
Figures













References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- C11496/A17786, C416/A21999/Cancer Research UK (CRUK)
- CTUQQR-DEC22/100009/CRUK_/Cancer Research UK/United Kingdom
- Young Investigator Grant/International Association for the Study of Lung Cancer (IASLC)
- 202060447/Japan Society for the Promotion of Science London (JSPS London)
- I4677/Austrian Science Fund (Fonds zur Förderung der Wissenschaftlichen Forschung)
- CC2041/WT_/Wellcome Trust/United Kingdom
- ID16584/Novo Nordisk Foundation Center for Basic Metabolic Research (NovoNordisk Foundation Center for Basic Metabolic Research)
- 220589/Z/20/Z/Wellcome Trust (Wellcome)
- EDDCPJT\100008/Cancer Research UK (CRUK)
- UCL/12/0279/University College London (UCL)
- Bolyai Research Scholarship/Hungarian Academy of Sciences | Magyar Tudományos Akadémia Számítástechnikai és Automatizálási Kutatóintézet (Számítástechnikai és Automatizálási Kutatóintézet)
LinkOut - more resources
Full Text Sources
Medical
