

Characterization and dosimetric predictors for absolute lymphocyte count changes during neoadjuvant chemoradiotherapy with or without pembrolizumab for esophageal squamous cell carcinoma: an analysis of a prospective cohort
- PMID: 39789555
- PMCID: PMC11720911
- DOI: 10.1186/s13014-024-02581-9
Characterization and dosimetric predictors for absolute lymphocyte count changes during neoadjuvant chemoradiotherapy with or without pembrolizumab for esophageal squamous cell carcinoma: an analysis of a prospective cohort
Abstract
Aim: To characterize the differences of dynamic changes for absolute lymphocyte count (ALC) among esophageal squamous cell carcinoma (ESCC) patients treated with neoadjuvant chemoradiotherapy (nCRT) with or without pembrolizumab, as well as to investigate the clinical and lymphocyte-related organs dosimetric parameters that would impact ALC nadir during nCRT.
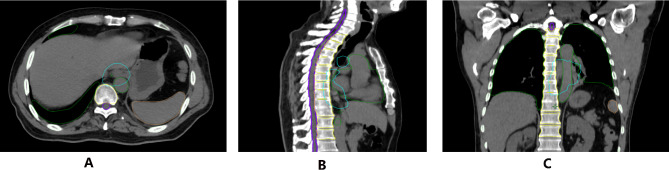
Materials and methods: A total of 216 ESCC patients who received nCRT (with pembrolizumab 144; without pembrolizumab: 72) were identified from a prospective cohort. Weekly and 1-month post-nCRT ALC were identified. lymphocyte-related organs at risk (LOARs) were delineated. linear and logistic regression analysis was used to analyze the association between G4 lymphopenia/lymphopenia nadir and clinical/DVHs factors. Receiver-operating characteristic curves were used to derive optimal dosimetric planning constraints. Grade 4 (G4) lymphopenia was defined as ALC < 0.2 × 109/L during nCRT.
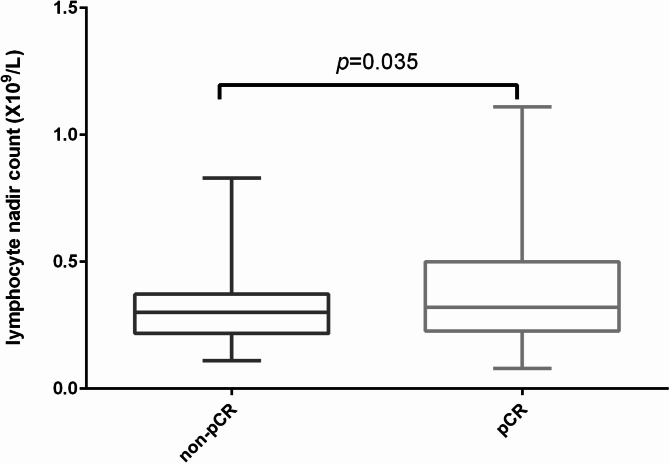
Results: G4 lymphopenia was observed in 35 ESCC patients (16.2%) during neoadjuvant treatment. Compared to nCRT alone, the addition of pembrolizumab to nCRT significantly improve lymphopenia recovery in the 1-months after nCRT (p = 0.0003), but the ALC at other time point during nCRT and ALC nadir was comparable between the two groups. A total of 198 patients finally received surgery. Of them, 98 patients archived pCR (49.5%), with 50.4% (68/135 patients) in nCRT with pembrolizumab and 47.6% (30/63) in nCRT alone(p = 0.94), respectively. The mean ALC nadir in the pCR group was significantly higher than those without (p = 0.0003). Multivariable linear and logistic regression analysis indicated that TVB mean dose, TVB V5, TVB V10, TVB V20, mean cardiopulmonary dose, mean ribs dose, mean whole body dose, mean spleen dose, V5, V10, and V20 of spleen dose were significantly associated with developing grade 4 lymphopenia. Dosimetric analysis showed that lymphocyte-sparing photon or proton irradiation was feasible while did not compromise clinically acceptable objectives.
Conclusion: The addition of pembrolizumab to nCRT improved lymphopenia recovery for ESCC after trimodality therapy. ALC nadir was significantly associated with pCR and RFS after nCRT. Sparing of LOARs using advanced radiation techniques might reduce the risk of developing lymphopenia and improve treatment response in the era of immunotherapy.
Keywords: Esophageal squamous cell carcinoma; Lymphocyte-related organs at risk; Neoadjuvant chemoradiotherapy; Pembrolizumab.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This study was approved by the Ethics Committee of Ruijin hospital, Shanghai Jiao Tong University School of Medicine. Competing interests: The authors declare no competing interests.
Figures


References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J Clin. 2021;71(3):209–49. - PubMed
-
- Hulscher JB, Tijssen JG, Obertop H, van Lanschot JJ. Transthoracic versus transhiatal resection for carcinoma of the esophagus: a meta-analysis. Ann Thorac Surg. 2001;72(1):306–13. - PubMed
-
- Cooper JS, Guo MD, Herskovic A, Macdonald JS, Martenson JA Jr., Al-Sarraf M, Byhardt R, Russell AH, Beitler JJ, Spencer S, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85–01). Radiation Therapy Oncol Group Jama. 1999;281(17):1623–7. - PubMed
-
- Eyck BM, van Lanschot JJB, Hulshof M, van der Wilk BJ, Shapiro J, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, van Laarhoven HWM, Nieuwenhuijzen GAP, et al. Ten-year outcome of neoadjuvant chemoradiotherapy plus surgery for esophageal cancer: the randomized controlled CROSS trial. J Clin Oncology: Official J Am Soc Clin Oncol. 2021;39(18):1995–2004. - PubMed
-
- Yang H, Liu H, Chen Y, Zhu C, Fang W, Yu Z, Mao W, Xiang J, Han Y, Chen Z et al. Long-term efficacy of neoadjuvant chemoradiotherapy plus surgery for the treatment of locally advanced esophageal squamous cell carcinoma: the NEOCRTEC5010 randomized clinical trial. JAMA surgery. 2021. 156(8):721–729. - PMC - PubMed
MeSH terms
Substances
Grants and funding
- 202340226/Clinical Research Special Project of Shanghai Municipal Health Commission Health Industry
- 23Y11904700/Shanghai Science and Technology Innovation Action Plan Medical Innovation Research Project
- 82102819/the National Science Foundation of China
- KC2021-JX-0170-9/Beijing Science and Technology Innovation Medical Development Foundation
- 23dz2261000/Shanghai Key Laboratory of Proton-therapy
LinkOut - more resources
Full Text Sources
Medical
