

Impact of rTMS and iTBS on Cerebral Hemodynamics and Swallowing in Unilateral Stroke: Insights from fNIRS
- PMID: 39789787
- PMCID: PMC11726903
- DOI: 10.12659/MSM.944521
Impact of rTMS and iTBS on Cerebral Hemodynamics and Swallowing in Unilateral Stroke: Insights from fNIRS
Abstract
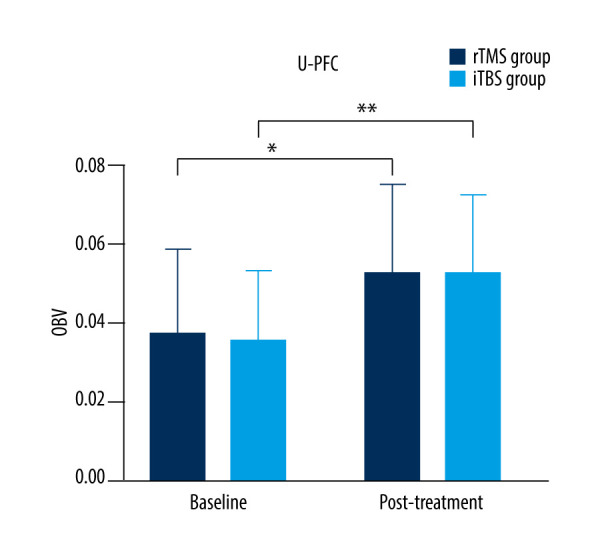
BACKGROUND Swallowing is a complex behavior involving the musculoskeletal system and higher-order brain functions. We investigated the effects of different modalities of repetitive transcranial magnetic stimulation (rTMS) on the unaffected hemisphere and observed correlation between suprahyoid muscle activity and cortical activation in unilateral stroke patients when swallowing saliva, based on functional near-infrared spectroscopy (fNIRS). MATERIAL AND METHODS From November 2022 to March 2023, twenty-five patients with unilateral stroke were screened using computed tomography or magnetic resonance imaging and identified via a video fluoroscopic swallow study. Finally, patients were divided into rTMS (n=10) and iTBS (n=10) groups. Both groups received 2 weeks of stimulation on unaffected suprahyoid motor cortex. Surface electromyographic measured peak amplitude and swallowing time of bilateral suprahyoid muscles, and penetration-aspiration scale was assessed at baseline and after treatment. fNIRS monitored oxyhemoglobin beta values (OBV) in the primary motor, sensory, and bilateral prefrontal cortex (PFC). RESULTS Both groups showed significant improvements in penetration-aspiration scale, peak amplitude, and swallowing time, compared with baseline (P<0.001), and increased OBV in unaffected regions (P<0.05), especially PFC (P<0.001). No significant OBV increases were seen in affected regions (P>0.05). After treatment, OBV in the unaffected PFC was significantly higher than in the unaffected primary sensory and motor cortex regions for both groups (P<0.05). No significant differences were observed between groups in outcome measures (P>0.05). CONCLUSIONS rTMS and iTBS significantly improved swallowing function in unilateral stroke, relying on compensation by the unaffected cortex, particularly the PFC. iTBS may outperform rTMS by shortening treatment sessions and improving efficiency.
Conflict of interest statement
Figures









References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
